You might also like
- Cardinal Health Lab Poc Rapid Diagnostics Catalog 2019 PDFDocument85 pagesCardinal Health Lab Poc Rapid Diagnostics Catalog 2019 PDFsiscaNo ratings yet
- Non Protein CompoundsDocument64 pagesNon Protein CompoundsAbigail Mayled LausNo ratings yet
- Immunity To MicrobesDocument25 pagesImmunity To MicrobestimcarasNo ratings yet
- Immune Disorders, Vaccines, Covid-19 and Drug Reactions DiscussedDocument73 pagesImmune Disorders, Vaccines, Covid-19 and Drug Reactions DiscussedErum JanNo ratings yet
- URIC ACID LyphoDocument2 pagesURIC ACID LyphoDharmesh Patel50% (2)
- A Theranostic and Precision Medicine Approach for Female-Specific CancersFrom EverandA Theranostic and Precision Medicine Approach for Female-Specific CancersRama Rao MallaNo ratings yet
- Factors Affecting Immune SystemDocument50 pagesFactors Affecting Immune SystemMa NuNo ratings yet
- ANA Profile 3Document20 pagesANA Profile 3vemalNo ratings yet
- Antinuclear Antibody TestDocument3 pagesAntinuclear Antibody TestElise Señadoza Aulmo-BarcenasNo ratings yet
- Blood Loss: Acute Chronic Inadequate Production of Normal Blood CellsDocument11 pagesBlood Loss: Acute Chronic Inadequate Production of Normal Blood CellsSheila Amor BodegasNo ratings yet
- Cc1 Lab Uric Acid Determination - CuenoDocument6 pagesCc1 Lab Uric Acid Determination - CuenoShyne ReyesNo ratings yet
- Salmonella, Shigella, Pseudomonas & Proteus IDDocument4 pagesSalmonella, Shigella, Pseudomonas & Proteus IDAmrit KoiralaNo ratings yet
- Autoimmune DiseasesDocument41 pagesAutoimmune DiseasesGanesh V GaonkarNo ratings yet
- Monoclonal Antibody: Engineering and TherapyDocument39 pagesMonoclonal Antibody: Engineering and TherapyAugusta Rizki AnandaNo ratings yet
- SEMINAR 1 - Autoimmune Diseases and Immunodeficiency DisordersDocument12 pagesSEMINAR 1 - Autoimmune Diseases and Immunodeficiency DisordersAprille PatolNo ratings yet
- Fana TrainingDocument174 pagesFana TrainingHaidee SaavedraNo ratings yet
- Elisa (Enzyme Linked Immunosorbant Assay)Document4 pagesElisa (Enzyme Linked Immunosorbant Assay)Linette GuillermoNo ratings yet
- Unit II Cells & Organs of ImmuneDocument69 pagesUnit II Cells & Organs of ImmuneSAMUELNo ratings yet
- Elisa: Enzyme-Linked Immunosorbent AssayDocument12 pagesElisa: Enzyme-Linked Immunosorbent AssayAmitNo ratings yet
- Mechanism of AutoimmunityDocument29 pagesMechanism of AutoimmunityMalliga SundareshanNo ratings yet
- Handouts Immune Defenses F11Document12 pagesHandouts Immune Defenses F11Kelly Trainor100% (1)
- Adjuvant breast cancer therapy agentsDocument3 pagesAdjuvant breast cancer therapy agentsGem BulaongNo ratings yet
- Q: How Common Are Autoimmune Diseases? ADocument12 pagesQ: How Common Are Autoimmune Diseases? AApplecart23No ratings yet
- Saumya Gupta Moderator: Dr. Vishal GuptaDocument41 pagesSaumya Gupta Moderator: Dr. Vishal Guptaimranqazi11No ratings yet
- General Features of The Immune SystemDocument6 pagesGeneral Features of The Immune SystemMinerva Bautista RoseteNo ratings yet
- Autoimmune Disorders: DR Muhammad ZUBAIR Consultant Chemical PathologistDocument52 pagesAutoimmune Disorders: DR Muhammad ZUBAIR Consultant Chemical PathologistZubair YousafNo ratings yet
- Metabolism of Vitamin DDocument36 pagesMetabolism of Vitamin DNisachon DenpraphaNo ratings yet
- Megaloblastic AnaemiaDocument11 pagesMegaloblastic AnaemiaJesmin_36No ratings yet
- Monoclonal Antibody Production: Hybridoma TechnologyDocument25 pagesMonoclonal Antibody Production: Hybridoma TechnologyAmzad pashaNo ratings yet
- 14.human GeneticsDocument18 pages14.human GeneticsRenjith Moorikkaran MNo ratings yet
- Immunology 2 - (Innate Immunity & Acquired Immunity)Document53 pagesImmunology 2 - (Innate Immunity & Acquired Immunity)hufflypink_95No ratings yet
- AAK ANA Komplett Kunde PDFDocument64 pagesAAK ANA Komplett Kunde PDFm parasiteNo ratings yet
- Introduction To ImmunologyDocument21 pagesIntroduction To Immunologysaeed5220020% (1)
- BiologyDocument27 pagesBiologyAnand GNo ratings yet
- 04 AntigenDocument30 pages04 AntigenVivin Syamsul ArifinNo ratings yet
- Hormonal ImbalanceDocument2 pagesHormonal Imbalanceapi-328485397No ratings yet
- CytokinesDocument12 pagesCytokinesclventuriniNo ratings yet
- Urinary Biomarkers For Prostate Cancer A ReviewDocument7 pagesUrinary Biomarkers For Prostate Cancer A ReviewIuliana FloreaNo ratings yet
- The Immune SystemDocument15 pagesThe Immune SystemAslak Torgersen100% (1)
- Organs of The Immune SystemDocument23 pagesOrgans of The Immune SystembandarosNo ratings yet
- Principles of serodiagnosis techniquesDocument26 pagesPrinciples of serodiagnosis techniquesNipun ShamikaNo ratings yet
- Apoptosis tutorial notes: Understanding programmed cell deathDocument8 pagesApoptosis tutorial notes: Understanding programmed cell deathismealNo ratings yet
- Crispr TechniqueDocument16 pagesCrispr TechniqueAmmar Abbas100% (1)
- Vitamins, minerals and trace elements essential guideDocument5 pagesVitamins, minerals and trace elements essential guideCristhian LozanoNo ratings yet
- Innate and Adaptive Immunity: Cells, Organs and FunctionsDocument17 pagesInnate and Adaptive Immunity: Cells, Organs and FunctionsBasma RagabNo ratings yet
- Antibiotic Sensitivity Tests: Roba Attar Dr. Nisreen TashkandiDocument48 pagesAntibiotic Sensitivity Tests: Roba Attar Dr. Nisreen TashkandiTriciaNo ratings yet
- Liver function tests: Van den Bergh test and assessment of secretory functionDocument7 pagesLiver function tests: Van den Bergh test and assessment of secretory functionadiNo ratings yet
- Ig Structuer and FunctionsDocument34 pagesIg Structuer and FunctionsDentist Dina SamyNo ratings yet
- Antineoplastic Agents 2011 Dental MARCH-1Document41 pagesAntineoplastic Agents 2011 Dental MARCH-1BinayakSwainNo ratings yet
- Gene therapy aims to treat cancer by altering faulty genesDocument7 pagesGene therapy aims to treat cancer by altering faulty genesesraa elsharkawyNo ratings yet
- AKC Histo Drawings PDFDocument130 pagesAKC Histo Drawings PDFDanDeleanuNo ratings yet
- Components of The Immune SystemDocument8 pagesComponents of The Immune Systemبراءة أحمد السلاماتNo ratings yet
- NPTEL – Cellular and Molecular Immunology: Antibodies and AntigensDocument33 pagesNPTEL – Cellular and Molecular Immunology: Antibodies and AntigensAygul RamankulovaNo ratings yet
- Biochemical Assessment of Vitamin DDocument24 pagesBiochemical Assessment of Vitamin DKarunya VkNo ratings yet
- 03 Adaptive Immune SystemDocument14 pages03 Adaptive Immune SystemEnea NastriNo ratings yet
- Cultivation Media For BacteriaDocument4 pagesCultivation Media For BacterialapetitefilleNo ratings yet
- Fat Soluble: Vitamins and Minerals Vitamins Vitamin Food Sources Health Benefit DeficiencyDocument2 pagesFat Soluble: Vitamins and Minerals Vitamins Vitamin Food Sources Health Benefit DeficiencyJthan ReyesNo ratings yet
- Humoral & Celullar ImmunityDocument60 pagesHumoral & Celullar ImmunityHaziq KamardinNo ratings yet
- Medical ParasitologyDocument53 pagesMedical ParasitologyCandilicious10No ratings yet
- Hematology Quick StudyDocument47 pagesHematology Quick StudyShanygne Krystal SwannNo ratings yet
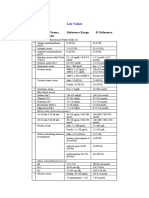
- Blood, Plasma, Serum Reference Range SI Reference: Lab ValuesDocument4 pagesBlood, Plasma, Serum Reference Range SI Reference: Lab ValuesEvaG2012No ratings yet
- Cancer Biology, a Study of Cancer Pathogenesis: How to Prevent Cancer and DiseasesFrom EverandCancer Biology, a Study of Cancer Pathogenesis: How to Prevent Cancer and DiseasesNo ratings yet
- 2015-2016 HandbookDocument93 pages2015-2016 HandbookrevaishNo ratings yet
- 2015-2016 HandbookDocument93 pages2015-2016 HandbookrevaishNo ratings yet
- What Population Health Means To MeDocument1 pageWhat Population Health Means To MerevaishNo ratings yet
- Creating BreakthroughDocument71 pagesCreating Breakthroughrevaish0% (1)
- How To Choose A Scientific ProblemDocument3 pagesHow To Choose A Scientific Problemblueradish450No ratings yet
- Biopolymer SDocument10 pagesBiopolymer SrevaishNo ratings yet
- Complete SyllabusDocument110 pagesComplete SyllabusrevaishNo ratings yet
- MathsDocument6 pagesMathsrevaishNo ratings yet
- Aids and Immunodeficiencies: - Kiruthika ManivannanDocument35 pagesAids and Immunodeficiencies: - Kiruthika ManivannanrevaishNo ratings yet
- Rheumatology MedicineDocument19 pagesRheumatology MedicineSami Ur RehmanNo ratings yet
- Absolute Dermatology Review - Mastering Clinical Conditions On The Dermatology Recertification Exam (PDFDrive)Document461 pagesAbsolute Dermatology Review - Mastering Clinical Conditions On The Dermatology Recertification Exam (PDFDrive)mogoscristina100% (1)
- Medical English skillsDocument56 pagesMedical English skillsFrancesca GrassiaNo ratings yet
- AntibioticsDocument7 pagesAntibioticsCeleste Largo Arayan-LedesmaNo ratings yet
- AMOS Revision PaedsDocument2 pagesAMOS Revision PaedsDeborah AnneNo ratings yet
- A New Discovery On Whats Causing ItchinessDocument7 pagesA New Discovery On Whats Causing ItchinessJackson D.S.No ratings yet
- Glomerular Disorders - Part I & Part II (ARI NOTES)Document144 pagesGlomerular Disorders - Part I & Part II (ARI NOTES)Laiba FatimaNo ratings yet
- Secure your family's future with this adjustable life insurance planDocument25 pagesSecure your family's future with this adjustable life insurance planaaaNo ratings yet
- Pleural Effusion - Pulmonary Disorders - MSD Manual Professional EditionDocument5 pagesPleural Effusion - Pulmonary Disorders - MSD Manual Professional EditionfaniNo ratings yet
- Systemic Lupus Erythematosus (Sle) : BSN 3 - 3 Group 2Document13 pagesSystemic Lupus Erythematosus (Sle) : BSN 3 - 3 Group 2Dianne BernardoNo ratings yet
- 35th Vicenza Course On Aki & CRRT: Selected Abstracts From TheDocument27 pages35th Vicenza Course On Aki & CRRT: Selected Abstracts From TheMARIA LEIVANo ratings yet
- Inflammatory ImmunologicDocument35 pagesInflammatory Immunologickaren dapalNo ratings yet
- DR HaifaDocument28 pagesDR HaifaAlex SamNo ratings yet
- A Comprehensive Guide For COVID-19 Longhaulers and Physicians - The PASC Master DocumentDocument24 pagesA Comprehensive Guide For COVID-19 Longhaulers and Physicians - The PASC Master DocumentVirginia Ferrer UrbanoNo ratings yet
- Lupus Thesis StatementDocument7 pagesLupus Thesis Statementaprilwatsonlittlerock100% (2)
- Liu, W., Shi, L., & Li, S. (2019) - The Immunomodulatory Effect of Alpha-Lipoic Acid in Autoimmune Diseases. BioMed Research InternationalDocument12 pagesLiu, W., Shi, L., & Li, S. (2019) - The Immunomodulatory Effect of Alpha-Lipoic Acid in Autoimmune Diseases. BioMed Research InternationalFelicia JesslynNo ratings yet
- Classification of Rheumatic DiseasesDocument29 pagesClassification of Rheumatic DiseasesBahaa Shaaban100% (5)
- Micro Lec Ars Sessions 17 23Document9 pagesMicro Lec Ars Sessions 17 23rica sebabillonesNo ratings yet
- Lec 21Document28 pagesLec 21Ukash sukarmanNo ratings yet
- Oral Lichenoid Lesions - Distinguishing The Benign From The Deadly (2017)Document14 pagesOral Lichenoid Lesions - Distinguishing The Benign From The Deadly (2017)JohnNo ratings yet
- Laboratory Investigations in RheumatologyDocument43 pagesLaboratory Investigations in RheumatologyBahaa Shaaban100% (1)
- Healing Declarations for Health and WellnessDocument2 pagesHealing Declarations for Health and WellnessLintu100% (1)
- (Mebooksfree - Net) Cas Stu Int Med 1stDocument159 pages(Mebooksfree - Net) Cas Stu Int Med 1stEjaz AhmedNo ratings yet
- 2-Autoimmune DiseasesDocument29 pages2-Autoimmune DiseasessoniaNo ratings yet
- Chapter 6 - Diseases of The Immune SystemDocument12 pagesChapter 6 - Diseases of The Immune SystemAgnieszka WisniewskaNo ratings yet
- 3.the Immune ResponseDocument135 pages3.the Immune ResponsebekaluNo ratings yet
- Jurnal Kedokteran Dan Kesehatan Indonesia: Association Between Malnutrition and StrokeDocument7 pagesJurnal Kedokteran Dan Kesehatan Indonesia: Association Between Malnutrition and StrokeAditya BatlajeryNo ratings yet
- Experimental Eye ResearchDocument10 pagesExperimental Eye ResearchApriansyah Arfandy AzisNo ratings yet