You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Jolly Phonics Activity Book 3 (Wwwlanguagecentre - 230920 - 122454Document37 pagesJolly Phonics Activity Book 3 (Wwwlanguagecentre - 230920 - 122454Nelly Fernandez100% (1)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Session 5 Phenphenomenolgy CtitiqueDocument22 pagesSession 5 Phenphenomenolgy CtitiqueNelly FernandezNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Case Study Rresearch - Design and MethodsDocument28 pagesCase Study Rresearch - Design and MethodsPriscila PenaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Session 5 Phenphenomenolgy CtitiqueDocument22 pagesSession 5 Phenphenomenolgy CtitiqueNelly FernandezNo ratings yet
- Research Methods - Session 5Document15 pagesResearch Methods - Session 5Nelly FernandezNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Session 2 - Research Methods - GlossaryDocument17 pagesSession 2 - Research Methods - GlossaryNelly FernandezNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Research Methods - Session 4Document13 pagesResearch Methods - Session 4Nelly FernandezNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Child Psych Lesson 1: Early DevelopmentDocument30 pagesChild Psych Lesson 1: Early DevelopmentNelly FernandezNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- TEACHING PRACTICE CLASSROOM TECHNIQUESDocument13 pagesTEACHING PRACTICE CLASSROOM TECHNIQUESNelly FernandezNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- What is phonicsDocument244 pagesWhat is phonicsNelly FernandezNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- What is phonicsDocument244 pagesWhat is phonicsNelly FernandezNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Solid Solution For Catalytic Ammonia Synthesis FromDocument8 pagesSolid Solution For Catalytic Ammonia Synthesis FromAhmad AlShahrourNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Phy 111 - Eos Exam 2015Document7 pagesPhy 111 - Eos Exam 2015caphus mazengeraNo ratings yet
- MTPDF4 Exact and Non-Exact Differential EquationsDocument27 pagesMTPDF4 Exact and Non-Exact Differential Equationsnaughty dela cruzNo ratings yet
- Lamosa CatalogoDocument51 pagesLamosa CatalogoSofi SamareitesNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Check List Valve PDFDocument2 pagesCheck List Valve PDFikan100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Trends and Fads in Business SVDocument2 pagesTrends and Fads in Business SVMarie-Anne DentzerNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- KNS 1063 Bending and Shear Stress AnalysisDocument11 pagesKNS 1063 Bending and Shear Stress AnalysisLuna LatisyaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Combination Meter: D1 (A), D2 (B)Document10 pagesCombination Meter: D1 (A), D2 (B)PeterNo ratings yet
- D 4 Development of Beam Equations: M X V XDocument1 pageD 4 Development of Beam Equations: M X V XAHMED SHAKERNo ratings yet
- Pore and Formation PressureDocument4 pagesPore and Formation PressureramadhanipdNo ratings yet
- Awareness On Biomedical Waste Management Among Dental Students - A Cross Sectional Questionnaire SurveyDocument8 pagesAwareness On Biomedical Waste Management Among Dental Students - A Cross Sectional Questionnaire SurveyIJAR JOURNALNo ratings yet
- BPSM Strategic Management ProcessDocument4 pagesBPSM Strategic Management ProcessFaiyaz panchbhayaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Lesson Plans For Class ObservationDocument7 pagesLesson Plans For Class ObservationArnel NavalesNo ratings yet
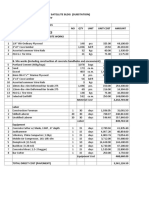
- PROPOSED ARFF BUILDINGDocument27 pagesPROPOSED ARFF BUILDINGDale Bryan S DalmacioNo ratings yet
- BG BG 202102080912862 User Manual - File (Long) BG BG-8Document1 pageBG BG 202102080912862 User Manual - File (Long) BG BG-8hofolo39No ratings yet
- Module 5 Greek ArchDocument22 pagesModule 5 Greek ArchKyla A. EstoestaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Simplified Coil DesignDocument6 pagesSimplified Coil DesignNestor Alberto EscalaNo ratings yet
- Danica Seleskovitch-Mariann A Lederer: Interpréter Pour TraduireDocument17 pagesDanica Seleskovitch-Mariann A Lederer: Interpréter Pour TraduireGarima KukrejaNo ratings yet
- John Constantine Rouge Loner Primordial Orphan Paranormal DetectiveDocument4 pagesJohn Constantine Rouge Loner Primordial Orphan Paranormal DetectiveMirko PrćićNo ratings yet
- An Approach To Predict The Failure of Water Mains Under Climatic VariationsDocument16 pagesAn Approach To Predict The Failure of Water Mains Under Climatic VariationsGeorge, Yonghe YuNo ratings yet
- CMO Olympiad Book For Class 3Document13 pagesCMO Olympiad Book For Class 3Srividya BaiNo ratings yet
- Teaching Strategies in The New NormalDocument19 pagesTeaching Strategies in The New NormalEloisa Canlas - Quizon67% (3)
- Python Quals PytestDocument4 pagesPython Quals PytestAnkit RathoreNo ratings yet
- Math Lesson on Completing PatternsDocument7 pagesMath Lesson on Completing PatternsJazmyne Obra100% (1)
- Stat and Prob Q1 M3Document15 pagesStat and Prob Q1 M3Samantha Kyle E. PedrigozaNo ratings yet
- Human Rights PDFDocument18 pagesHuman Rights PDFRohitNo ratings yet
- Hot and Cold CorrosionDocument6 pagesHot and Cold CorrosioniceburnerNo ratings yet
- PreviewpdfDocument68 pagesPreviewpdfwong alusNo ratings yet
- Gathering Statistical DataDocument8 pagesGathering Statistical DataianNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Towards Innovative Community Building: DLSU Holds Henry Sy, Sr. Hall GroundbreakingDocument2 pagesTowards Innovative Community Building: DLSU Holds Henry Sy, Sr. Hall GroundbreakingCarl ChiangNo ratings yet