You might also like
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Endocrinology - Review NotesDocument9 pagesEndocrinology - Review NotesRoa Al-SajjanNo ratings yet
- Drug Management of Diabetes MellitusDocument36 pagesDrug Management of Diabetes MellitusHassan.shehri100% (15)
- Diabetes Management ATIDocument15 pagesDiabetes Management ATIJessica ChirinoNo ratings yet
- Pharmacology Review NotesDocument24 pagesPharmacology Review NotescampbellqueenNo ratings yet
- Insulin Initiation and Intensification in Type 2 DiabetesDocument54 pagesInsulin Initiation and Intensification in Type 2 DiabetesAshraf Shaaban MahfouzNo ratings yet
- Insulin Secretion and FunctionDocument8 pagesInsulin Secretion and FunctionWendy EscalanteNo ratings yet
- Diabetes Melitus IIDocument8 pagesDiabetes Melitus IIharunnuranNo ratings yet
- Fisika - Physics For High SchoolDocument396 pagesFisika - Physics For High SchoolZainal AbidinNo ratings yet
- Standards PoolsDocument26 pagesStandards PoolsKimMyPatZaNo ratings yet
- DM Ppt. NewDocument26 pagesDM Ppt. NewRio Ramon HilarioNo ratings yet
- Basal Bolus InsulinDMT22009Document92 pagesBasal Bolus InsulinDMT22009scribdNo ratings yet
- Diabetic Management Update, Hospitalyzed To Daily Care - Dr. Supriyanto Kartodarsono, SPPDDocument48 pagesDiabetic Management Update, Hospitalyzed To Daily Care - Dr. Supriyanto Kartodarsono, SPPDEcank RsmrNo ratings yet
- 6wa Retrofit GuideDocument13 pages6wa Retrofit GuideAnonymous X5q33TQ100% (1)
- Diabetes Insulin InitiationDocument12 pagesDiabetes Insulin InitiationSatinder BhallaNo ratings yet
- Business Plan For Mobile Food CourtDocument13 pagesBusiness Plan For Mobile Food CourtMd. Al- AminNo ratings yet
- April 2016Document4 pagesApril 2016Albert CorderoNo ratings yet
- BPM Governance Platform Progress Business ProcessDocument22 pagesBPM Governance Platform Progress Business ProcessLando ReyesNo ratings yet
- Internship Project Report on MathematicsDocument18 pagesInternship Project Report on MathematicsNancini AVNo ratings yet
- Insulin Initiation PPT - PPTX 2Document53 pagesInsulin Initiation PPT - PPTX 2Meno Ali100% (1)
- Glycemic ManagementDocument39 pagesGlycemic ManagementZayar HmunNo ratings yet
- DiabetesMellitisChap09 SpecialPopulationsDocument12 pagesDiabetesMellitisChap09 SpecialPopulationsarmandoNo ratings yet
- Thera L15 PracticalDocument21 pagesThera L15 PracticalFatmaNo ratings yet
- Inpatient Management of Diabetes MellitusDocument38 pagesInpatient Management of Diabetes Mellitusmsala76No ratings yet
- 8.0 Acute Complications of Diabetes: 8.1 RecommendationsDocument5 pages8.0 Acute Complications of Diabetes: 8.1 RecommendationsAdriana Roa BallesterosNo ratings yet
- DM Lab 2 - FinalDocument33 pagesDM Lab 2 - FinalMahamed Wefkey OmranNo ratings yet
- CHAPTER 7 - Inpatient Management of Diabetes and HyperglycemiaDocument6 pagesCHAPTER 7 - Inpatient Management of Diabetes and HyperglycemiaenesNo ratings yet
- What To Do When Your Patient Has Diabetes: Karen A. Mcdonough MD Inpatient Medical Service UwmcDocument45 pagesWhat To Do When Your Patient Has Diabetes: Karen A. Mcdonough MD Inpatient Medical Service UwmchemanjaliNo ratings yet
- Managing Diabetes in HospitalsDocument9 pagesManaging Diabetes in HospitalsJharaNo ratings yet
- Inpatient Guideline JoslinDocument8 pagesInpatient Guideline Joslinospinu6780No ratings yet
- Gestational DiabetesDocument51 pagesGestational Diabeteskhadzx100% (2)
- Case Study DiabetesDocument15 pagesCase Study DiabetessamanNo ratings yet
- Peran Perawat DLM Rawat Inap DMDocument57 pagesPeran Perawat DLM Rawat Inap DMMuhidin AeNo ratings yet
- Clinical Practice Guidelines For The Inpatient Management of Diabetes/Hypergylcemia in AdultsDocument4 pagesClinical Practice Guidelines For The Inpatient Management of Diabetes/Hypergylcemia in AdultselexboyNo ratings yet
- Pharmacotherapy - Diabetes II - Dr. Mohammed KamalDocument46 pagesPharmacotherapy - Diabetes II - Dr. Mohammed KamalMohammed KamalNo ratings yet
- Management of Gestational DiabetesDocument3 pagesManagement of Gestational DiabetesNazia SalmanNo ratings yet
- CPG Diabetes MellitusDocument66 pagesCPG Diabetes MellitusBrian BeeNo ratings yet
- Insulin Protocols J Krinsley Rev July 2011Document1 pageInsulin Protocols J Krinsley Rev July 2011Nuha AL-YousfiNo ratings yet
- Guidelines For DiabetesDocument43 pagesGuidelines For Diabeteskashiftdr100% (1)
- Management of Severe Ulcerative Colitis: DR - Siddharth SinghDocument21 pagesManagement of Severe Ulcerative Colitis: DR - Siddharth SinghLohith VakacherlaNo ratings yet
- Glycemic control in hospitalized patientsDocument31 pagesGlycemic control in hospitalized patientsahmed_g_salihNo ratings yet
- Dr.Rihab Pediatrics 02.Pediatric DM Part TwoDocument7 pagesDr.Rihab Pediatrics 02.Pediatric DM Part TwoMujtaba JawadNo ratings yet
- Meglitinide Works by Stimulating The Release of Insulin in The Presence of GlucoseDocument53 pagesMeglitinide Works by Stimulating The Release of Insulin in The Presence of GlucoseWil LesterNo ratings yet
- Outdoor & Indoor Treatment of Diabetes MellitusDocument8 pagesOutdoor & Indoor Treatment of Diabetes MellitusDR. PRITHWIRAJ MAITINo ratings yet
- Guideline, Management of HypoglycemiaDocument5 pagesGuideline, Management of HypoglycemianellieauthorNo ratings yet
- Quality Tip - ADA Guideline Updates - 2010: Diagnosis of DiabetesDocument7 pagesQuality Tip - ADA Guideline Updates - 2010: Diagnosis of Diabetesyunitaekawati1459No ratings yet
- Insulin GNTDocument41 pagesInsulin GNTV Narayan Rao TummalaNo ratings yet
- Diabetes in Special PopulationDocument33 pagesDiabetes in Special PopulationhidayatNo ratings yet
- Pharmaceutical Care in Dm. Apoteker UbayaDocument48 pagesPharmaceutical Care in Dm. Apoteker UbayaViona PrasetyoNo ratings yet
- Management of T1DMDocument21 pagesManagement of T1DMSaurabh AgrawalNo ratings yet
- Diabetes Cases: Nahda College Program of Pharmacy Department of Clinical Pharmacy 2020-2021Document23 pagesDiabetes Cases: Nahda College Program of Pharmacy Department of Clinical Pharmacy 2020-2021Basil DomiNo ratings yet
- Target Range For Glycemic Control: 80-140 MG/DL (Generally 110 MG/DL)Document3 pagesTarget Range For Glycemic Control: 80-140 MG/DL (Generally 110 MG/DL)Otchi Pudtrie Wijaya100% (1)
- GDM Screening Test and ManagementDocument5 pagesGDM Screening Test and ManagementTan Yuet YangNo ratings yet
- Surgery in Diabetes Mellitus (DM) : Walid Sayed Abdelkader Hassanen Specialist of Internal MedicineDocument18 pagesSurgery in Diabetes Mellitus (DM) : Walid Sayed Abdelkader Hassanen Specialist of Internal Medicineanand787No ratings yet
- Samba Consensus For Diabetes During Ambulatory SurgeryDocument5 pagesSamba Consensus For Diabetes During Ambulatory Surgeryabirray65No ratings yet
- Executive Summary RSSDI Recommendations 241019Document44 pagesExecutive Summary RSSDI Recommendations 241019Sunil MishraNo ratings yet
- DM Medical Nutritional TherapyDocument5 pagesDM Medical Nutritional TherapyNeil AlviarNo ratings yet
- AMB PBLD 2 - Management of The Diabetic Patient Presenting For Ambulatory Surgery - InstructorDocument8 pagesAMB PBLD 2 - Management of The Diabetic Patient Presenting For Ambulatory Surgery - InstructorhvNo ratings yet
- Insulin Dosing For Fat and ProteinDocument19 pagesInsulin Dosing For Fat and Proteinapi-356625183No ratings yet
- CH 39 Anaesthesia and Diabetes MellitusDocument6 pagesCH 39 Anaesthesia and Diabetes MellitusChristian LeepoNo ratings yet
- Diabetes Management in The Inpt SettingDocument3 pagesDiabetes Management in The Inpt Settingapi-648401824No ratings yet
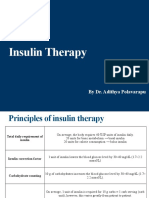
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- Diabetic EssayDocument6 pagesDiabetic Essayreet kaurNo ratings yet
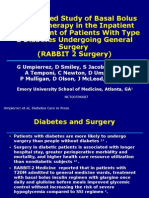
- RABBIT-2 Surgery - (12 - 2010)Document32 pagesRABBIT-2 Surgery - (12 - 2010)aromerozNo ratings yet
- Summary of IMBR-Saud Alzahrani-08-2020Document30 pagesSummary of IMBR-Saud Alzahrani-08-2020AHMAD ALROWAILYNo ratings yet
- Diabetic Nephropathy: Landmark Clinical TrialsDocument45 pagesDiabetic Nephropathy: Landmark Clinical TrialsTRP TSYONo ratings yet
- Mechanical Ventilation Settings for COVID-19Document3 pagesMechanical Ventilation Settings for COVID-19Carlos ZepedaNo ratings yet
- Mechanical Ventilation Waveform Analysis for COVID-19Document4 pagesMechanical Ventilation Waveform Analysis for COVID-19Carlos ZepedaNo ratings yet
- Management Specific To COVID-19Document7 pagesManagement Specific To COVID-19Carlos ZepedaNo ratings yet
- Introduction To Mechanical Ventilation PDFDocument7 pagesIntroduction To Mechanical Ventilation PDFCarlos ZepedaNo ratings yet
- Extubation: Mechanical Ventilation For COVID-19Document7 pagesExtubation: Mechanical Ventilation For COVID-19Carlos ZepedaNo ratings yet
- Daily Assessment of PatientsDocument9 pagesDaily Assessment of PatientsCarlos ZepedaNo ratings yet
- Patient Positioning During AnaesthesiaDocument6 pagesPatient Positioning During AnaesthesiaDarman ZulfikarNo ratings yet
- Xray Film Reading Made EasyyyyyDocument158 pagesXray Film Reading Made EasyyyyyyudhistiraoneNo ratings yet
- Acquisition of SharesDocument3 pagesAcquisition of SharesChaudhary Mohsin RazaNo ratings yet
- Cis Bin Haider GRP LTD - HSBC BankDocument5 pagesCis Bin Haider GRP LTD - HSBC BankEllerNo ratings yet
- Key Benefits of Cloud-Based Internet of Vehicle (IoV) - Enabled Fleet Weight Management SystemDocument5 pagesKey Benefits of Cloud-Based Internet of Vehicle (IoV) - Enabled Fleet Weight Management SystemVelumani sNo ratings yet
- Bhushan Steel LTD (BHUS IN) - Balance SheetDocument4 pagesBhushan Steel LTD (BHUS IN) - Balance SheetVamsi GunturuNo ratings yet
- Ir 2101Document14 pagesIr 2101Willard DmpseyNo ratings yet
- Menomonee Falls Express News 091413Document32 pagesMenomonee Falls Express News 091413Hometown Publications - Express NewsNo ratings yet
- 5 Basic Model of PorterDocument6 pages5 Basic Model of PorterJahanvi PandyaNo ratings yet
- Ari Globe Valve SupraDocument26 pagesAri Globe Valve SupraAi-samaNo ratings yet
- DRW Questions 2Document16 pagesDRW Questions 2Natasha Elena TarunadjajaNo ratings yet
- Re-registering a vehicle in Karnataka - A step-by-step guideDocument4 pagesRe-registering a vehicle in Karnataka - A step-by-step guideHidayathulla HasanNo ratings yet
- Nevada Reports 1882-1883 (17 Nev.) PDFDocument334 pagesNevada Reports 1882-1883 (17 Nev.) PDFthadzigsNo ratings yet
- JohnsonJohnson 2006 PDFDocument84 pagesJohnsonJohnson 2006 PDFakfar b417No ratings yet
- Indexed Addressing & Flow Rate AveragingDocument5 pagesIndexed Addressing & Flow Rate AveragingMestrecal MeloNo ratings yet
- ICICI Health Insurance Policy DetailsDocument3 pagesICICI Health Insurance Policy DetailsarjunNo ratings yet
- Flexible Instruction Delivery Plan Template CONTENT 5Document2 pagesFlexible Instruction Delivery Plan Template CONTENT 5Edward Barber100% (3)
- Adb Doc Easa Reliance 8 Centerline Stopbar Declaracao de Conformidade EasaDocument2 pagesAdb Doc Easa Reliance 8 Centerline Stopbar Declaracao de Conformidade Easagiant360No ratings yet
- Affidavit Defends Wife's InnocenceDocument6 pagesAffidavit Defends Wife's InnocenceGreggy LawNo ratings yet
- Local Govt & Public Corp CasesDocument4 pagesLocal Govt & Public Corp CasesAngel OlaNo ratings yet
- The Bank and The Mundhra AffairDocument14 pagesThe Bank and The Mundhra AffairAmbika MehrotraNo ratings yet
- Digest Office of The Ombudsman V Samaniego 2008Document3 pagesDigest Office of The Ombudsman V Samaniego 2008Lea Gabrielle FariolaNo ratings yet
- CIVL 222 AXIAL MEMBERSDocument27 pagesCIVL 222 AXIAL MEMBERSskhan247100% (1)
- Lab Exercise 3 SoilScie Group4Document10 pagesLab Exercise 3 SoilScie Group4Jhunard Christian O. AsayasNo ratings yet
- 12.CEH Module 3 Assignment 3.1Document7 pages12.CEH Module 3 Assignment 3.1piyuhNo ratings yet
- Henry FordDocument18 pagesHenry Fordsonabeta07No ratings yet