You might also like
- Jourdain - Music The Brain and EcstasyDocument6 pagesJourdain - Music The Brain and EcstasyHamedNahavandiNo ratings yet
- The Brain: Our Universe WithinDocument7 pagesThe Brain: Our Universe WithinSally Morem67% (3)
- (Basics (Birkhauser) (Book 1) ) Ulrich Exner - Basics Spatial Design (Basics (Birkhauser) ) (2004, Birkhäuser Architecture) - Libgen - LiDocument90 pages(Basics (Birkhauser) (Book 1) ) Ulrich Exner - Basics Spatial Design (Basics (Birkhauser) ) (2004, Birkhäuser Architecture) - Libgen - LiAfework MerahiNo ratings yet
- Neurology pdf-1Document142 pagesNeurology pdf-1Ahmed Adel SaadNo ratings yet
- Osteopathic Structural ExamDocument27 pagesOsteopathic Structural ExamFernando100% (1)
- Geriatric Considerations in Nursing Anp AssignmentDocument12 pagesGeriatric Considerations in Nursing Anp AssignmentLIDIYA MOL P V50% (2)
- Correlative Neuroanatomy of The Sensory SystemDocument8 pagesCorrelative Neuroanatomy of The Sensory SystemJonathan Gorospe100% (2)
- The Composition of Electroacoustic Music: by Rodolfo CaesarDocument72 pagesThe Composition of Electroacoustic Music: by Rodolfo CaesarDaríoNowakNo ratings yet
- Neurological AssessmentDocument82 pagesNeurological AssessmentSan Shine100% (1)
- Neuro Examination (Auto-Saved)Document18 pagesNeuro Examination (Auto-Saved)MALIK WASEEM ABBASNo ratings yet
- Neurological Examination 3Document46 pagesNeurological Examination 3VIKAS PUNIANo ratings yet
- Neurological Examination Part 2Document120 pagesNeurological Examination Part 24 Strings to EcstasyNo ratings yet
- Upper & Lower Limb ExaminationDocument20 pagesUpper & Lower Limb Examinationcvmqx7yppd100% (1)
- Motor TestingDocument58 pagesMotor Testingsarguss14100% (2)
- Neurologic AssessmentDocument98 pagesNeurologic AssessmentJona Kristin EnclunaNo ratings yet
- Neurological History and ExaminationDocument30 pagesNeurological History and ExaminationMaria Agatha100% (1)
- Neurological Health AssessmentDocument63 pagesNeurological Health AssessmentAhmed ElryahNo ratings yet
- Introductory Lecture, Neurological Examination: General OverviewDocument8 pagesIntroductory Lecture, Neurological Examination: General OverviewmustafaNo ratings yet
- Sensory ExamDocument24 pagesSensory Examsarguss14100% (2)
- Nervous System Reflexes and Senses: Physiology Lab-4 October, 2018Document21 pagesNervous System Reflexes and Senses: Physiology Lab-4 October, 2018Madhu LodhiNo ratings yet
- Cerebral PalsyDocument36 pagesCerebral PalsyZulaikha Fadzil100% (1)
- Neurology: by Dennis Jason Alcantara, RN, USRN, MAN CanDocument213 pagesNeurology: by Dennis Jason Alcantara, RN, USRN, MAN CanKristel-Mia Dimalanta RamosNo ratings yet
- Care of Clients With Neurologic DisordersDocument78 pagesCare of Clients With Neurologic DisordersKatri ArasaNo ratings yet
- Cerebellar Function Tests: Experiment 29: Md-1C Group 5Document42 pagesCerebellar Function Tests: Experiment 29: Md-1C Group 5Verlette Roselle Aguisanda LizardoNo ratings yet
- Cerebellar DisordersDocument51 pagesCerebellar DisorderswasimNo ratings yet
- Combo Upper Lesions 5th YearDocument55 pagesCombo Upper Lesions 5th YearJane SharpsNo ratings yet
- Spinal Cord Injury: Emergency NursingDocument36 pagesSpinal Cord Injury: Emergency NursingJaya Tanujaya OttoNo ratings yet
- SCIENCEDocument51 pagesSCIENCEDrmohamed Kamel MahranNo ratings yet
- WA0044.encDocument40 pagesWA0044.encmalfed adrianoNo ratings yet
- Neurovascular Assessment.... MMMMMDocument7 pagesNeurovascular Assessment.... MMMMMArian May MarcosNo ratings yet
- Neurologic ExaminationDocument67 pagesNeurologic Examinationሀይደር ዶ.ር100% (1)
- Exercise 4: Motor Control Systems: ABST-1L Group 2 Dimaculangan, Quintana, Reyes, Santos, VillaosDocument38 pagesExercise 4: Motor Control Systems: ABST-1L Group 2 Dimaculangan, Quintana, Reyes, Santos, VillaosofficialpatdeeNo ratings yet
- Assessment of The Musculo-Skeletal SystemDocument46 pagesAssessment of The Musculo-Skeletal SystemRaquel M. MendozaNo ratings yet
- Physical Assessment MSK Level 3 2019Document93 pagesPhysical Assessment MSK Level 3 2019Daniela OrtalNo ratings yet
- Cerebellar DisordersDocument29 pagesCerebellar DisordersArslan Aslam100% (1)
- Motor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistDocument36 pagesMotor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistJim Jose Antony100% (1)
- Motor ExaminationDocument36 pagesMotor ExaminationKenneth DizonNo ratings yet
- Principles of Musculoskeletal Assessment: Introduction To Clinical Studies Traumatology RHS 231 Dr. Einas Al-EisaDocument36 pagesPrinciples of Musculoskeletal Assessment: Introduction To Clinical Studies Traumatology RHS 231 Dr. Einas Al-EisaroshinisureshNo ratings yet
- Assessment of Sensory SystemDocument21 pagesAssessment of Sensory SystemDr. SyedaNo ratings yet
- Neuro-Coordination Umair PTDocument20 pagesNeuro-Coordination Umair PTFatima SeharNo ratings yet
- Neural MobilizationDocument50 pagesNeural MobilizationPRIYAM XEROXNo ratings yet
- File 1694763811 0005620 SpasticityDocument17 pagesFile 1694763811 0005620 Spasticity2022824838.pasangNo ratings yet
- 10.neurological Assessment Cont...Document33 pages10.neurological Assessment Cont...Chenii RoyNo ratings yet
- The Neurological ExaminationDocument53 pagesThe Neurological ExaminationApolinar González Hernández100% (2)
- Chapter 18: NeurologyDocument22 pagesChapter 18: NeurologypoddataNo ratings yet
- Reflex Physiologis: DR Sugianto Sps Mkes PHDDocument31 pagesReflex Physiologis: DR Sugianto Sps Mkes PHDRian Kurniawan LaksonoNo ratings yet
- Anesthetic MonitoringDocument11 pagesAnesthetic Monitoring102022No ratings yet
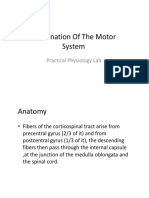
- Examination of The Motor System: Practical Physiology LabDocument20 pagesExamination of The Motor System: Practical Physiology Labحسين سعد حاتم خضيرNo ratings yet
- Disorders of The Tone: - Hitesh Rohit (3 Year B.P.T.)Document43 pagesDisorders of The Tone: - Hitesh Rohit (3 Year B.P.T.)Hitesh RohitNo ratings yet
- Examination of The Sensory SystemDocument37 pagesExamination of The Sensory SystemRobin RajNo ratings yet
- Sensory, Motor & Integration SystemsDocument82 pagesSensory, Motor & Integration SystemsAnonymous JBhe5iDqHNo ratings yet
- Neurological Assessment PDFDocument52 pagesNeurological Assessment PDFJosephine George JojoNo ratings yet
- Motor System: Zhao Xinyu Department of Neurology The First Affiliated Hospital of Zhengzhou UniversityDocument33 pagesMotor System: Zhao Xinyu Department of Neurology The First Affiliated Hospital of Zhengzhou Universityapi-19916399No ratings yet
- Musculoskeletal SystemDocument5 pagesMusculoskeletal SystemDale Ros CollamatNo ratings yet
- SensoryDocument24 pagesSensoryBeta Wattimena100% (1)
- Sensation: General Considerations Prior To EvaluationDocument12 pagesSensation: General Considerations Prior To EvaluationbenznakupNo ratings yet
- Neurological AssessmentDocument76 pagesNeurological Assessmentjcabatit3No ratings yet
- Examination of Central Nervous SystemDocument85 pagesExamination of Central Nervous SystemdrbhawnavermaNo ratings yet
- CerebellumDocument32 pagesCerebellumDr VirenNo ratings yet
- Assessment of The Musclo-Skletal SystemDocument25 pagesAssessment of The Musclo-Skletal SystemjacnpoyNo ratings yet
- Draft 1Document33 pagesDraft 1RasYa DINo ratings yet
- Neurological Eval SensoryDocument25 pagesNeurological Eval SensoryAyen FornollesNo ratings yet
- Mitland For Cevical SpineDocument52 pagesMitland For Cevical SpineMohamed RamadanNo ratings yet
- Proprioception, Vestibular & CoordinationDocument28 pagesProprioception, Vestibular & Coordinationzm2h8hpsq8No ratings yet
- ReflexesDocument22 pagesReflexesgmpcbpzdysNo ratings yet
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Jaques Dalcroze S Music Based Rhythmic Training Affects Gait Parameters and Quality of Life in Parkinson S Disease 11687Document19 pagesJaques Dalcroze S Music Based Rhythmic Training Affects Gait Parameters and Quality of Life in Parkinson S Disease 11687Raghu NadhNo ratings yet
- Tools and ScalesDocument47 pagesTools and ScalesRaghu NadhNo ratings yet
- NHM Spmu Recruitment Notification 2020Document6 pagesNHM Spmu Recruitment Notification 2020Raghu NadhNo ratings yet
- Cancerandexercise 161004225344Document30 pagesCancerandexercise 161004225344Raghu NadhNo ratings yet
- Provisional Merit List For The Post Code: 1 - ConsultantsDocument73 pagesProvisional Merit List For The Post Code: 1 - ConsultantsRaghu NadhNo ratings yet
- Brain TDocument27 pagesBrain TRaghu NadhNo ratings yet
- No Data FoundDocument1 pageNo Data FoundRaghu NadhNo ratings yet
- DR M Ushashree 1 Yr PG Gandhi Medical CollegeDocument58 pagesDR M Ushashree 1 Yr PG Gandhi Medical CollegeRaghu NadhNo ratings yet
- Tendon Transfers and Upper Limb Disorders: Aws KhanfarDocument41 pagesTendon Transfers and Upper Limb Disorders: Aws KhanfarRaghu NadhNo ratings yet
- Autonomic Nervous System Testing: By: Murtaza Neurophysiology DeptDocument41 pagesAutonomic Nervous System Testing: By: Murtaza Neurophysiology DeptRaghu NadhNo ratings yet
- Guidance On Rapid Antibody Test Kits For Covid-19: S. No. Name of Company Name of Kit Lot No./batch NoDocument2 pagesGuidance On Rapid Antibody Test Kits For Covid-19: S. No. Name of Company Name of Kit Lot No./batch NoRaghu NadhNo ratings yet
- Issuance of SC or ST CertificatesDocument32 pagesIssuance of SC or ST CertificatesRaghu NadhNo ratings yet
- MPT-1st Year 19pDocument19 pagesMPT-1st Year 19pRaghu Nadh50% (2)
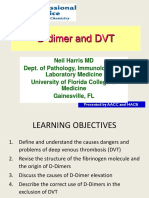
- CTH D Dimers May 2 2013 PDFDocument42 pagesCTH D Dimers May 2 2013 PDFRaghu NadhNo ratings yet
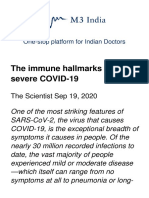
- The Immune Hallmarks of Severe CovidDocument30 pagesThe Immune Hallmarks of Severe CovidRaghu NadhNo ratings yet
- NSAA Only ManualVersion-2.0 May-2017Document19 pagesNSAA Only ManualVersion-2.0 May-2017Raghu NadhNo ratings yet
- Egen Klassifikation Scale Version 2 (EK2) Steffensen 2008Document2 pagesEgen Klassifikation Scale Version 2 (EK2) Steffensen 2008Raghu NadhNo ratings yet
- MPTH Thesis Topic List 2010 - : Name of The Student Department Name of Thesis Topic StatusDocument6 pagesMPTH Thesis Topic List 2010 - : Name of The Student Department Name of Thesis Topic StatusRaghu NadhNo ratings yet
- Somatosensory System: G.Arvelandze N.MalashkhiaDocument26 pagesSomatosensory System: G.Arvelandze N.MalashkhialuckyNo ratings yet
- You: Clothes-Body-Clothes Series and Sensorial Masks in 1967 While Working As AnDocument8 pagesYou: Clothes-Body-Clothes Series and Sensorial Masks in 1967 While Working As Anmyhr0107No ratings yet
- A Preliminary Investigation of The Relationship Between Sensory Processing and Social Play in Autism Spectrum DisorderDocument9 pagesA Preliminary Investigation of The Relationship Between Sensory Processing and Social Play in Autism Spectrum DisorderPaulinaNo ratings yet
- Accepted Manuscript: Urgen KonczakDocument16 pagesAccepted Manuscript: Urgen KonczakRun CapNo ratings yet
- Reading IeltsDocument5 pagesReading IeltsjohnlycasNo ratings yet
- P10 Goran Šimić: 3. Studeni 2020. ZagrebDocument26 pagesP10 Goran Šimić: 3. Studeni 2020. ZagrebGoran SimicNo ratings yet
- 3.1 ABC's of SensationDocument6 pages3.1 ABC's of SensationMary MzButterflyy SmithNo ratings yet
- The-Physical-Examination-and-Health-Assessment 2Document3 pagesThe-Physical-Examination-and-Health-Assessment 2Christian Jewel GambolNo ratings yet
- Arts Appreciation ReviewerDocument5 pagesArts Appreciation ReviewerbrylleNo ratings yet
- Haptic Vibrotactile Trigger Technology Disrupting The Neuromatrix To Reduce Pain Severity and InterferenceDocument7 pagesHaptic Vibrotactile Trigger Technology Disrupting The Neuromatrix To Reduce Pain Severity and InterferenceEriNo ratings yet
- In Touch Hand Therapy HandoutDocument1 pageIn Touch Hand Therapy Handouthullaballoo3697No ratings yet
- Presentation On How To Heal Toxic ThoughtsDocument3 pagesPresentation On How To Heal Toxic ThoughtsКсюша ДейNo ratings yet
- Module 2 Sensory DetailsDocument5 pagesModule 2 Sensory DetailsCharlieNo ratings yet
- Speech & Language Therapy in Practice, Summer 2005Document32 pagesSpeech & Language Therapy in Practice, Summer 2005Speech & Language Therapy in PracticeNo ratings yet
- Unconciounsness & Sensory DepDocument92 pagesUnconciounsness & Sensory DepSimran SimzNo ratings yet
- Bodily SelfDocument22 pagesBodily SelfGaetano CaliendoNo ratings yet
- ImageryDocument35 pagesImageryJose Ramon CarlosNo ratings yet
- SIPTDocument2 pagesSIPTAthila Mohamed100% (1)
- Hum121 - D2 ImageryDocument9 pagesHum121 - D2 ImageryShiela Mae CruzNo ratings yet
- Eskin Seminar ReportDocument18 pagesEskin Seminar ReportKalyan HvNo ratings yet
- Assessment Checklist On Different ChildDocument15 pagesAssessment Checklist On Different ChildRuth WellNo ratings yet
- Brain and Cranial NervesDocument111 pagesBrain and Cranial NervesAnonymous m9wRhxF4d100% (2)
- TACTILEDocument43 pagesTACTILELatitude 28 GalleryNo ratings yet
- Assessment of Upper Extremity Impairment Function and ActivityDocument28 pagesAssessment of Upper Extremity Impairment Function and ActivityLakshmi PrasannaNo ratings yet