You might also like
- Neuroscience - 4.3 - Examination of Cerebellar Systems and Meninges (KSD)Document4 pagesNeuroscience - 4.3 - Examination of Cerebellar Systems and Meninges (KSD)Kevin C. AguilarNo ratings yet
- Co-Ordination: Prepared by Ahmed Shawky AliDocument59 pagesCo-Ordination: Prepared by Ahmed Shawky Alivenkata ramakrishnaiahNo ratings yet
- Cerebellar DisordersDocument51 pagesCerebellar DisorderswasimNo ratings yet
- Neurological History and ExaminationDocument30 pagesNeurological History and ExaminationMaria Agatha100% (1)
- Motor Neuron Disease.Document38 pagesMotor Neuron Disease.sanjana sangleNo ratings yet
- Cerebellar SyndromesDocument10 pagesCerebellar SyndromesEmi Valcov100% (1)
- Cranial Nerve Exam Part 1Document9 pagesCranial Nerve Exam Part 1Jennifer Pisco LiracNo ratings yet
- Transverse MyelitisDocument19 pagesTransverse MyelitisAnonymous YHQmN8a01100% (1)
- Elbow Special TestDocument4 pagesElbow Special TestEllaiza Astacaan100% (1)
- Movement Disorders BabcockDocument19 pagesMovement Disorders BabcockBaiq Trisna SatrianaNo ratings yet
- Cranial Neuropathies Guide: Electrodiagnosis and ManagementDocument74 pagesCranial Neuropathies Guide: Electrodiagnosis and ManagementKevin Woodard100% (1)
- Understanding Movement DisordersDocument54 pagesUnderstanding Movement DisordersIhda ParidahNo ratings yet
- Upper and Lower Motor NeuronDocument28 pagesUpper and Lower Motor NeuronDr Abdullah SubhanNo ratings yet
- Diseases of The Spinal CordDocument89 pagesDiseases of The Spinal CordLolla SinwarNo ratings yet
- Oculomotor Nerve: Components Main Action SuppliesDocument10 pagesOculomotor Nerve: Components Main Action Suppliesdisha1990No ratings yet
- Hip ExaminationDocument84 pagesHip ExaminationDeepak KumarNo ratings yet
- LMN VS UmnDocument10 pagesLMN VS UmnyosuaNo ratings yet
- Deep Tendon Reflex Examination GuideDocument4 pagesDeep Tendon Reflex Examination GuideDan Ali100% (1)
- Ataxias Neuro Condition DetailedDocument80 pagesAtaxias Neuro Condition DetailedMikail AtiyehNo ratings yet
- Muscles of the Scapula and ShoulderDocument6 pagesMuscles of the Scapula and ShoulderAndika Anjani AgustinNo ratings yet
- Myopathies: Lecture ObjectivesDocument15 pagesMyopathies: Lecture ObjectivesanjelikaNo ratings yet
- Neuroscience Board ReviewDocument216 pagesNeuroscience Board ReviewRafael TerceiroNo ratings yet
- Spinal Cord Disease by GadisaDocument128 pagesSpinal Cord Disease by GadisaGadisa DejeneNo ratings yet
- Classification of Upper Limb Orthosis: Presented To: Miss Soonhan Rani Presented By: Syeda Zoha Hassan TaqviDocument16 pagesClassification of Upper Limb Orthosis: Presented To: Miss Soonhan Rani Presented By: Syeda Zoha Hassan Taqvizoha hassanNo ratings yet
- NCS EMG Procedure DesrciptionDocument13 pagesNCS EMG Procedure DesrciptionShauki AliNo ratings yet
- Vestibular Disorders and Rehab GuideDocument15 pagesVestibular Disorders and Rehab GuideMehul RathoreNo ratings yet
- What Is PolymyositisDocument24 pagesWhat Is PolymyositisAshraf MobyNo ratings yet
- Muscle Origin Insertion Innervation Action: (Branch of The Brachial Plexus)Document58 pagesMuscle Origin Insertion Innervation Action: (Branch of The Brachial Plexus)sdfs sdfdNo ratings yet
- Exercise ECGDocument85 pagesExercise ECGSUHER ANUNo ratings yet
- Neuro AssessmentDocument23 pagesNeuro AssessmentSidra aliNo ratings yet
- Study Guide NeurophysiologyDocument2 pagesStudy Guide NeurophysiologyAndrew MajorNo ratings yet
- Cervical PalpationDocument22 pagesCervical Palpationpraveen100% (12)
- Test, Questions and Clinical - Cases in NeurologyDocument111 pagesTest, Questions and Clinical - Cases in NeurologyPurwa Rane100% (1)
- Approach To VertigoDocument16 pagesApproach To VertigolubaA5No ratings yet
- Traction: Cervical & LumbarDocument21 pagesTraction: Cervical & LumbarBoud ElhassanNo ratings yet
- Upper Extremity AnatomyDocument1 pageUpper Extremity AnatomyKristineNo ratings yet
- Tx3: Bobath'S Neurodevelopmental Treatment: PT Applications Team DLSMHSI CRS PT Department AY 2018-2019Document4 pagesTx3: Bobath'S Neurodevelopmental Treatment: PT Applications Team DLSMHSI CRS PT Department AY 2018-2019Pauline JaleaNo ratings yet
- D. Brainstem: PONS (Ventral Metencephalon) 1. External Consideration A. Ventral ViewDocument39 pagesD. Brainstem: PONS (Ventral Metencephalon) 1. External Consideration A. Ventral ViewMarvic SueltoNo ratings yet
- Knee Joint Structure and FunctionDocument16 pagesKnee Joint Structure and FunctionSiva ShanmugamNo ratings yet
- Biomechanics of Peripheral and Spinal Nerve RootsDocument86 pagesBiomechanics of Peripheral and Spinal Nerve RootsJawad HassanNo ratings yet
- Lumbar Spine AssessmentDocument26 pagesLumbar Spine Assessmentyoyo_pt2007100% (1)
- Wrist and Hand ComplexDocument6 pagesWrist and Hand ComplexAlyssa Mae CamposanoNo ratings yet
- Juvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDDocument38 pagesJuvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDLavi GoyalNo ratings yet
- Bed Mobility and Positioning Exercises for Hemiplegic PatientsDocument133 pagesBed Mobility and Positioning Exercises for Hemiplegic Patientsktin17100% (1)
- ASIA Impairment ScaleDocument10 pagesASIA Impairment Scaleazimahzainal211No ratings yet
- Neuro - PathophysiologyDocument107 pagesNeuro - Pathophysiologyjmosser100% (4)
- Neurology Important McqsDocument12 pagesNeurology Important McqsFarhan Khosa100% (1)
- PNS Examination 15Document17 pagesPNS Examination 15NolanNo ratings yet
- SpondylosisDocument20 pagesSpondylosisLiza Puspita SariNo ratings yet
- Coordination AssessmentDocument30 pagesCoordination AssessmentBhawna PalNo ratings yet
- LMNL Vs UmnlDocument49 pagesLMNL Vs UmnlLohshini ManickavasagamNo ratings yet
- Quiz IVDocument5 pagesQuiz IVErvin T MileNo ratings yet
- Arm, Forearm, Hand MuscleDocument18 pagesArm, Forearm, Hand MusclerabeyaNo ratings yet
- Neurological AssessmentDocument64 pagesNeurological AssessmentNEuRoLoGisT CoFFeeCuP95% (20)
- Peripheral Nerve Injuries Classification and TreatmentDocument85 pagesPeripheral Nerve Injuries Classification and TreatmentSyed Abudaheer100% (3)
- Ascending TractsDocument42 pagesAscending TractsJustine Nyangaresi100% (2)
- Bicipital TendonitisDocument2 pagesBicipital TendonitisJ Cheung100% (2)
- Avascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAvascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (2)
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Ds 5344Document1 pageDs 5344Arslan AslamNo ratings yet
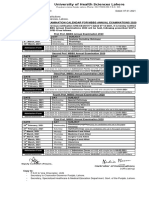
- University of Health Sciences, Lahore: Date SheetDocument1 pageUniversity of Health Sciences, Lahore: Date SheetArslan AslamNo ratings yet
- University of Health Sciences, Lahore: Date SheetDocument1 pageUniversity of Health Sciences, Lahore: Date SheetArslan AslamNo ratings yet
- Ds 5344Document1 pageDs 5344Arslan AslamNo ratings yet
- Ds 5344Document1 pageDs 5344Arslan AslamNo ratings yet
- All Affiliated Medical Institutions University of Health Sciences, LahoreDocument1 pageAll Affiliated Medical Institutions University of Health Sciences, LahoreArslan AslamNo ratings yet
- Locomotor TrainingDocument32 pagesLocomotor TrainingArslan AslamNo ratings yet
- Traumatic Brain Injury Part 1Document60 pagesTraumatic Brain Injury Part 1Arslan AslamNo ratings yet
- CONTROL OF MOVEMENT THEORIESDocument33 pagesCONTROL OF MOVEMENT THEORIESArslan Aslam100% (3)
- Physical Therapy Intervention in StrokeDocument26 pagesPhysical Therapy Intervention in StrokeArslan AslamNo ratings yet
- Degenerative and Progressive Central Nervous System DisordersDocument24 pagesDegenerative and Progressive Central Nervous System DisordersArslan AslamNo ratings yet
- Multiple Sclerosis: Saadia Perwaiz, PT BSPT, M. Phil-MskDocument39 pagesMultiple Sclerosis: Saadia Perwaiz, PT BSPT, M. Phil-MskArslan Aslam100% (2)
- Orthopantomography (: Orthopantograph or OPG)Document4 pagesOrthopantomography (: Orthopantograph or OPG)Arslan Aslam100% (1)
- Guillain-Barré Syndrome: Causes, Symptoms, TreatmentDocument26 pagesGuillain-Barré Syndrome: Causes, Symptoms, TreatmentArslan AslamNo ratings yet
- Medical Imaging X Ray RadiograhyDocument20 pagesMedical Imaging X Ray RadiograhyArslan AslamNo ratings yet
- DPT Lecture 1 RadiologyDocument22 pagesDPT Lecture 1 RadiologyArslan AslamNo ratings yet
- Fluoro DSA ContrastDocument20 pagesFluoro DSA ContrastArslan AslamNo ratings yet
- MammographyDocument10 pagesMammographyArslan AslamNo ratings yet
- Fungal Infections of The LungsDocument163 pagesFungal Infections of The Lungsmeaza rorisaNo ratings yet
- Rough Draft FinalDocument12 pagesRough Draft Finalapi-451554067No ratings yet
- COMPLETE BLOOD PICTURE Ok-1 PDFDocument78 pagesCOMPLETE BLOOD PICTURE Ok-1 PDFEmanuel100% (1)
- A Guide To The Treatment of Pressure UlcersDocument5 pagesA Guide To The Treatment of Pressure UlcersMac Perez LopezNo ratings yet
- Toddler & Preschooler NutritionDocument59 pagesToddler & Preschooler NutritionEka Laras0% (1)
- DS (Fenofibrate)Document5 pagesDS (Fenofibrate)Mary April MendezNo ratings yet
- Dry Dandruff With Meaning and PictureDocument3 pagesDry Dandruff With Meaning and PictureMargie Ballesteros ManzanoNo ratings yet
- 17-Year-Old Man With Sudden Left Testicular PainDocument20 pages17-Year-Old Man With Sudden Left Testicular PainnurisumirizqiNo ratings yet
- Differential Leukocyte Count:: The Types of LeukocytesDocument4 pagesDifferential Leukocyte Count:: The Types of LeukocytesSuandiNo ratings yet
- PRD Recomm PharmanexDocument2 pagesPRD Recomm PharmanexVioleta NaghiuNo ratings yet
- Medical Abbreviation Terms-2Document7 pagesMedical Abbreviation Terms-2Jmarie Brillantes PopiocoNo ratings yet
- BF Checklist EnglishDocument1 pageBF Checklist EnglishYwagar YwagarNo ratings yet
- Parent Ver SCH 0 6yrsDocument2 pagesParent Ver SCH 0 6yrsunmundoextranopodcastNo ratings yet
- Dietary Advice For Patients Taking OrlistatDocument12 pagesDietary Advice For Patients Taking OrlistatteddypolNo ratings yet
- Penatalaksanaan CAPDocument31 pagesPenatalaksanaan CAPridhoNo ratings yet
- Typhoid Fever and Paratyphoid Fever Are Lif1Document14 pagesTyphoid Fever and Paratyphoid Fever Are Lif1Cherry Ann DomingoNo ratings yet
- Nutrients: Protein Nutrition and Malnutrition in CKD and ESRDDocument19 pagesNutrients: Protein Nutrition and Malnutrition in CKD and ESRDrandy_27995No ratings yet
- Homeopathic Treatment For Arthritis May 11Document2 pagesHomeopathic Treatment For Arthritis May 11debprasNo ratings yet
- Diabecon Himalaya PDFDocument20 pagesDiabecon Himalaya PDFMulayam Singh YadavNo ratings yet
- Case021 57F PolymyalgiaDocument12 pagesCase021 57F PolymyalgiaHui YingNo ratings yet
- Jazul Lang MalakasDocument5 pagesJazul Lang MalakasDarl VelardeNo ratings yet
- Ceftriaxone Med CardDocument2 pagesCeftriaxone Med CardAnja de VriesNo ratings yet
- Rapini DermatopatologíaDocument474 pagesRapini DermatopatologíadrNo ratings yet
- Unit-4 SIR QUTEDocument28 pagesUnit-4 SIR QUTECapper RuedaNo ratings yet
- Pcap - PathophysiologyDocument4 pagesPcap - PathophysiologyAyla Mar100% (1)
- ANSWER Chapter II-Vocabulary ExerciseDocument4 pagesANSWER Chapter II-Vocabulary Exerciseberliana CahyaNo ratings yet
- Nbme 29 Questions (200) Done 211Document200 pagesNbme 29 Questions (200) Done 211Shahzeen Sajid KhanNo ratings yet
- Iot in HealthcareDocument6 pagesIot in Healthcareapi-297434994No ratings yet
- Potassium and HypertensionDocument5 pagesPotassium and HypertensionSheyla Alegre ParionaNo ratings yet
- Herbal PlantsDocument17 pagesHerbal PlantsCarl Angelo Santiago100% (1)