You might also like
- Oscc CmeDocument97 pagesOscc CmeKernYen LeeNo ratings yet
- Case StudyDocument10 pagesCase StudyMuhamad LukmanNo ratings yet
- Amenoria AssignmentDocument10 pagesAmenoria AssignmentBaihaqiNo ratings yet
- NEEDLE PRICK INJURY PREVENTION AND TREATMENTDocument8 pagesNEEDLE PRICK INJURY PREVENTION AND TREATMENTRizal FarieNo ratings yet
- Institut Latihan Kementerian Kesihatan Malaysia Johor BahruDocument9 pagesInstitut Latihan Kementerian Kesihatan Malaysia Johor BahruFardzli MatjakirNo ratings yet
- CarbuncleDocument14 pagesCarbuncleMohd Anuar IbrahimNo ratings yet
- Case Clerking HerniaDocument13 pagesCase Clerking Herniaamirun100% (1)
- Physical Examination of Orthopedic Patients: Dr. M. Bayu, Sp. OTDocument55 pagesPhysical Examination of Orthopedic Patients: Dr. M. Bayu, Sp. OTsurya gunawanNo ratings yet
- Mental Health Services in Malaysia: Past, Present and FutureDocument2 pagesMental Health Services in Malaysia: Past, Present and FutureCt Sapiah100% (1)
- Antiemetics & Oral Rehydration Salts (ORS)Document60 pagesAntiemetics & Oral Rehydration Salts (ORS)Saha DirllahNo ratings yet
- Gastric Case ClerkingDocument19 pagesGastric Case ClerkingAnelkaLouisNo ratings yet
- Institut Latihan Kementerian Kesihatan Malaysia: Nama PelatihDocument12 pagesInstitut Latihan Kementerian Kesihatan Malaysia: Nama PelatihIkmal HakimiNo ratings yet
- First ResponderDocument19 pagesFirst ResponderKimGaryNo ratings yet
- SellulitisDocument16 pagesSellulitisLanNo ratings yet
- Clerking Guide Obstetrics CasesDocument3 pagesClerking Guide Obstetrics CasesNorFarah Fatin AnuarNo ratings yet
- WHO 2013 PPH HighlightsDocument4 pagesWHO 2013 PPH HighlightsNimeJi B'leaf 윤 재No ratings yet
- Knowledge, Attitude and Practice of Mothers Regarding Neonatal Jaundice: A Hospital Based Observational StudyDocument3 pagesKnowledge, Attitude and Practice of Mothers Regarding Neonatal Jaundice: A Hospital Based Observational StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Kes StudyDocument17 pagesKes StudyMellCy L'sNo ratings yet
- Etika Pemakaian PPEDocument18 pagesEtika Pemakaian PPEasmintuyunNo ratings yet
- Malaysian Triage Category GuideDocument11 pagesMalaysian Triage Category GuideMUHAMMAD FAIZ BIN NASIR / HPUPM100% (1)
- Erpoc CmeDocument20 pagesErpoc CmeSharon J StephenNo ratings yet
- Polyhydramnios Sem5Document9 pagesPolyhydramnios Sem5Siti Nur AmirahNo ratings yet
- Anti-Gout AgentDocument42 pagesAnti-Gout AgentSaha DirllahNo ratings yet
- 1st Stage Labour LatestDocument24 pages1st Stage Labour Latestlieynna4996100% (2)
- CFCSDocument77 pagesCFCSNurul NadiahNo ratings yet
- CME AnaemiaDocument40 pagesCME AnaemiaNini Shuhaida Mat HarunNo ratings yet
- Case Clerking Tommeh FormatDocument13 pagesCase Clerking Tommeh FormatatNo ratings yet
- Pediatrics CWU Year 5Document7 pagesPediatrics CWU Year 5anon_67984147No ratings yet
- Exclusive Breastfeeding Among Nursing MotherDocument7 pagesExclusive Breastfeeding Among Nursing MotherOlowolafe SamuelNo ratings yet
- Abdominal Pain and ConstipationDocument14 pagesAbdominal Pain and ConstipationSelvat ThankamonyNo ratings yet
- Intraosseous and Arterial Line Access.1 - ArvindDocument27 pagesIntraosseous and Arterial Line Access.1 - ArvindArvind Qumar ThivakaranNo ratings yet
- Formulari Ubat KKM 3/2012Document238 pagesFormulari Ubat KKM 3/2012afiq83100% (3)
- Roster Wad 4 - 2018Document51 pagesRoster Wad 4 - 2018ramuoodooNo ratings yet
- Professional liability standards for medical negligenceDocument3 pagesProfessional liability standards for medical negligenceHo Wen HuiNo ratings yet
- Act 436 Midwives Act 1966Document20 pagesAct 436 Midwives Act 1966Adam Haida & CoNo ratings yet
- Case Clerking ETUDocument14 pagesCase Clerking ETUafiqah farizNo ratings yet
- Keabnormalan Kongenital (Hipospadias, Epispadias, Fimosis, Parafimosis, Undescended TestisDocument54 pagesKeabnormalan Kongenital (Hipospadias, Epispadias, Fimosis, Parafimosis, Undescended TestisSuriana KadirNo ratings yet
- Malaysian Triage Category-GreenDocument2 pagesMalaysian Triage Category-GreenArnold Daniel100% (3)
- Clerking An o & G CaseDocument57 pagesClerking An o & G CaseAlan Na100% (2)
- SELLULITISDocument16 pagesSELLULITISeizairie100% (4)
- Etiology PPPDocument24 pagesEtiology PPPCresty Estalilla100% (1)
- Knowledge of Glasgow Coma Scale Among ADEC StudentsDocument62 pagesKnowledge of Glasgow Coma Scale Among ADEC Students07 FARAH ATHIRAH BINTI MOH FUZINo ratings yet
- Case Clerking KunangDocument9 pagesCase Clerking KunangOtaiKatiNo ratings yet
- Nasogastric Tube InsertionDocument18 pagesNasogastric Tube InsertionSandya PallapotuNo ratings yet
- 2.7.1 C - Peranan Dan Tanggungjawab PPPDocument19 pages2.7.1 C - Peranan Dan Tanggungjawab PPPbobby redland0% (1)
- Detecting Increased Intracranial Pressure in a 6-Year-Old with Head InjuryDocument7 pagesDetecting Increased Intracranial Pressure in a 6-Year-Old with Head InjuryAuni Akif Aleesa100% (1)
- Clerking Case ExampleDocument2 pagesClerking Case ExampleUpdesh Singh0% (2)
- Apex BeatDocument23 pagesApex BeatDaniel Johnson100% (1)
- Duodenal Atresia, Volvulus, and IntussusceptionDocument15 pagesDuodenal Atresia, Volvulus, and IntussusceptionUndead LuciferNo ratings yet
- Clinical Approach to HypertensionDocument16 pagesClinical Approach to HypertensionShradha KhuranaNo ratings yet
- Stoke Fall PrecautionDocument31 pagesStoke Fall Precautionsmartie_chai100% (1)
- Edward SyndromeDocument11 pagesEdward SyndromeVikneswaran VîçkýNo ratings yet
- Bronchiol AsthmaDocument11 pagesBronchiol AsthmaMohd IzwanNo ratings yet
- Senarai Semak Troli KecemasanDocument2 pagesSenarai Semak Troli Kecemasanarnol309050% (4)
- Pain Management F05Document19 pagesPain Management F05Aneka DeanNo ratings yet
- Abg, FB, FBC, Buse, GXMDocument20 pagesAbg, FB, FBC, Buse, GXMeden_kampungboyNo ratings yet
- O&G Long Case Exam QuestionDocument21 pagesO&G Long Case Exam Questionwhee182No ratings yet
- Examination of rape victimDocument30 pagesExamination of rape victimfahadqazifreelancerNo ratings yet
- Oscc 21 Nov 2023Document50 pagesOscc 21 Nov 2023Normalinda YaacobNo ratings yet
- EXAMINATION OF RAPE VICTIM: GUIDELINES AND PROTOCOLSDocument27 pagesEXAMINATION OF RAPE VICTIM: GUIDELINES AND PROTOCOLSpreetNo ratings yet
- M.aqeef SummaryDocument4 pagesM.aqeef SummaryMagdalene ChooNo ratings yet
- Guide to Palliative MedicineDocument176 pagesGuide to Palliative MedicineMagdalene ChooNo ratings yet
- Management Guide With Table of ContentsDocument38 pagesManagement Guide With Table of ContentsMagdalene ChooNo ratings yet
- Compulsory Optional Emergency CVSDocument5 pagesCompulsory Optional Emergency CVSMagdalene ChooNo ratings yet
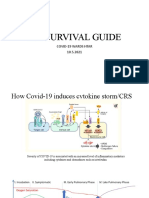
- Mo Survival Guide Covid HtarDocument26 pagesMo Survival Guide Covid HtarMagdalene ChooNo ratings yet
- Midazolam Is Used For Sedation (Endoscopic Procedures, Induction of Anesthesia, SedationDocument2 pagesMidazolam Is Used For Sedation (Endoscopic Procedures, Induction of Anesthesia, SedationMagdalene ChooNo ratings yet
- RAPID SEQUENCE INTUBATION (RSI) PROCEDUREDocument12 pagesRAPID SEQUENCE INTUBATION (RSI) PROCEDUREMagdalene ChooNo ratings yet
- Compilation of QuestionsDocument2 pagesCompilation of QuestionsMagdalene ChooNo ratings yet
- Rds CBL CombinedDocument37 pagesRds CBL CombinedMagdalene ChooNo ratings yet
- Lesson 3 - Violence in SportsDocument42 pagesLesson 3 - Violence in SportsJoyce Espenida SañanoNo ratings yet
- VakalatnamaDocument1 pageVakalatnamasyed suleman shahNo ratings yet
- 09PersonalProtectiveEquipment IOGP577version1.2Document2 pages09PersonalProtectiveEquipment IOGP577version1.2Ismail SultanNo ratings yet
- DLA Piper Offer of Employment A Guidance Note and Template Offer LetterDocument4 pagesDLA Piper Offer of Employment A Guidance Note and Template Offer LetterEzhilarasan NatarajanNo ratings yet
- Security Program and PoliciesDocument28 pagesSecurity Program and PoliciesMohammad IrfanNo ratings yet
- Not Stamped - Combined MotionDocument41 pagesNot Stamped - Combined MotionUSA TODAY Network100% (1)
- REMREVETHICS LMT - MCMPDocument28 pagesREMREVETHICS LMT - MCMPElla CardenasNo ratings yet
- Commentary of Ethiopian Agency LawDocument28 pagesCommentary of Ethiopian Agency LawWudneh DegeleNo ratings yet
- Lesson 4 Laws On Partnership and CorporationDocument34 pagesLesson 4 Laws On Partnership and CorporationGerstene Reynoso MaurNo ratings yet
- Willful failure to pay just debts grounds for disciplinary action against public officialsDocument16 pagesWillful failure to pay just debts grounds for disciplinary action against public officialsDarcyNo ratings yet
- Module 1Document11 pagesModule 1Mandanas GabrielNo ratings yet
- 09 Laboratory Exercise 1Document2 pages09 Laboratory Exercise 1JackDaniels TVNo ratings yet
- LBP vs. DalautaDocument1 pageLBP vs. DalautazaneNo ratings yet
- Development Strategies for Dalit Empowerment and InclusionDocument17 pagesDevelopment Strategies for Dalit Empowerment and InclusionluckybwinNo ratings yet
- Argumentative Essay AbortionDocument2 pagesArgumentative Essay Abortion• •ZaraYtMeteor• •No ratings yet
- People V Yanson DumancasDocument2 pagesPeople V Yanson DumancasMario MorenoNo ratings yet
- Copy Right and Neighboring RightsDocument48 pagesCopy Right and Neighboring RightsSiddarth Sunkari100% (2)
- Myrtle Beach Mayor and Council Squash Motion To Compel in Superblock TakeoverDocument6 pagesMyrtle Beach Mayor and Council Squash Motion To Compel in Superblock TakeoverMyrtleBeachSC newsNo ratings yet
- PNB vs. Cedo (1995)Document2 pagesPNB vs. Cedo (1995)DAblue ReyNo ratings yet
- Paz Reyes Aguam Vs CADocument1 pagePaz Reyes Aguam Vs CARaiza SunggayNo ratings yet
- Business LawDocument8 pagesBusiness LawANANYA SAININo ratings yet
- Case-Law and The Development of International Law Contributions by International Courts and Tribunals (Patrícia Galvão Teles (Editor) Etc.)Document289 pagesCase-Law and The Development of International Law Contributions by International Courts and Tribunals (Patrícia Galvão Teles (Editor) Etc.)Sovanrangsey KongNo ratings yet
- P.D. No. 657Document2 pagesP.D. No. 657CheerrylouuNo ratings yet
- Unit Ii AdrDocument112 pagesUnit Ii AdrShohan100% (1)
- 7610Document1 page7610ashNo ratings yet
- G.R. No. 208091 _ People v. MolejonDocument9 pagesG.R. No. 208091 _ People v. Molejonavy kamille buyuccanNo ratings yet
- Holsey-Hyman Investigation Letter - FinalDocument3 pagesHolsey-Hyman Investigation Letter - FinalJane PorterNo ratings yet
- Please Sign The Model Release You Requested FDocument2 pagesPlease Sign The Model Release You Requested FZuelviana VindhaNo ratings yet
- Marlin Daniels Vs Tarus Mack JudgementDocument6 pagesMarlin Daniels Vs Tarus Mack JudgementCharles FrazierNo ratings yet
- Memorial RespondentDocument38 pagesMemorial Respondentmanoj kumarNo ratings yet