You might also like
- Psychedelics Today - Trip Integration Journal PDFDocument190 pagesPsychedelics Today - Trip Integration Journal PDFGood Vibes80% (5)
- Waihou Marae Hireage Form With Amendments 15 March 2014Document2 pagesWaihou Marae Hireage Form With Amendments 15 March 2014api-53822848No ratings yet
- Purchasing and Commissioning of AutoclaveDocument28 pagesPurchasing and Commissioning of Autoclavenorhafizahstoh89100% (2)
- Mantoux Test: Pirquet Test, or PPD Test For Purified Protein Derivative) Is A Diagnostic Tool ForDocument5 pagesMantoux Test: Pirquet Test, or PPD Test For Purified Protein Derivative) Is A Diagnostic Tool ForGurmeet SinghNo ratings yet
- Test Bank For Pharmacology Principles and Applications 2nd Edition by FulcherDocument8 pagesTest Bank For Pharmacology Principles and Applications 2nd Edition by Fulchera493312980No ratings yet
- Preoperative Preparation of Patient For SurgeryDocument23 pagesPreoperative Preparation of Patient For SurgeryFauzi SebunyaNo ratings yet
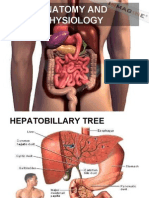
- Principles of Anatomy and Physiology: 14 EditionDocument62 pagesPrinciples of Anatomy and Physiology: 14 EditionWilliam C Chisha100% (1)
- Cardiovascular System: K. Hariharan Iv Eee - 'B'Document33 pagesCardiovascular System: K. Hariharan Iv Eee - 'B'Hari Haran100% (1)
- Study Guide PNS and CNSDocument7 pagesStudy Guide PNS and CNSsquicciariniNo ratings yet
- Unit 13 Endocrine GlandDocument73 pagesUnit 13 Endocrine GlandChandan ShahNo ratings yet
- Nervous SystemDocument22 pagesNervous SystemAltaf Hussain Khan50% (2)
- Anti Psychotic DrugsDocument67 pagesAnti Psychotic DrugsAhmed Osman100% (1)
- CNS - Limbic SystemDocument46 pagesCNS - Limbic SystemsarvinaNo ratings yet
- Patient Controlled AnalgesiaDocument35 pagesPatient Controlled AnalgesiamochkurniawanNo ratings yet
- Disorders of Posterior Pituitary GlandDocument21 pagesDisorders of Posterior Pituitary GlandCharlz ZipaganNo ratings yet
- Med SurDocument107 pagesMed Surapi-239934742No ratings yet
- Endo 3 Notes PDFDocument9 pagesEndo 3 Notes PDFDilNo ratings yet
- Nervous System: Chapter # 7Document69 pagesNervous System: Chapter # 7saddam ud dinNo ratings yet
- Anti Malarial DrugsDocument107 pagesAnti Malarial DrugsSindile MchunuNo ratings yet
- L - 2 Physiology of Respiration IIDocument25 pagesL - 2 Physiology of Respiration IIkaukab azimNo ratings yet
- ErythropoisisDocument47 pagesErythropoisisDisha SuvarnaNo ratings yet
- Body TissuesDocument29 pagesBody TissuesPurplesmilezNo ratings yet
- Depolarizing Muscle RelaxantDocument40 pagesDepolarizing Muscle RelaxantMohammad HayajnehNo ratings yet
- Premedication: Moderator: DR - Dinesh Kaushal Presentsd By: DR Rajesh Raman & DR Gopal SinghDocument60 pagesPremedication: Moderator: DR - Dinesh Kaushal Presentsd By: DR Rajesh Raman & DR Gopal Singhramanrajesh83No ratings yet
- The Human Nervous Syste1Document10 pagesThe Human Nervous Syste1taytay321No ratings yet
- Chemo ReceptorDocument8 pagesChemo ReceptorCheryl Lyn SanchezNo ratings yet
- Asthama & COPDDocument84 pagesAsthama & COPDAbdullah BhattiNo ratings yet
- Pharmacology: General Anaesthetic AgentsDocument65 pagesPharmacology: General Anaesthetic AgentsSharifa DarayanNo ratings yet
- Endocrine SystemDocument31 pagesEndocrine Systemsalmeohenzgabry100% (1)
- Study Guide QuestionsDocument4 pagesStudy Guide QuestionszaidaNo ratings yet
- Distribution of DrugsDocument36 pagesDistribution of DrugsKashar SaeedNo ratings yet
- AntihistaminesDocument66 pagesAntihistaminesAfif Bastian100% (1)
- Assignment AnesthesiaDocument9 pagesAssignment AnesthesiaRavi PatelNo ratings yet
- Adult BLSDocument50 pagesAdult BLSdianNo ratings yet
- Psychosocial Aspect of PainDocument21 pagesPsychosocial Aspect of PainLaiba WarisNo ratings yet
- Endocrine System 2017Document28 pagesEndocrine System 2017cyber sec100% (1)
- Breathing System: Assembly and Functional Analysis: DR Ashutosh Verma Moderator-Dr ChetnaDocument79 pagesBreathing System: Assembly and Functional Analysis: DR Ashutosh Verma Moderator-Dr Chetnaaahutosh vermaNo ratings yet
- Anatomy of Nervous SystemDocument26 pagesAnatomy of Nervous Systemrey martinoNo ratings yet
- Anatomy and Physiology of The Endocrine System: Presenté ParDocument64 pagesAnatomy and Physiology of The Endocrine System: Presenté ParYackson FrankNo ratings yet
- Human Anatomy,: First Edition Mckinley & O'LoughlinDocument40 pagesHuman Anatomy,: First Edition Mckinley & O'LoughlinAgung PurmanaNo ratings yet
- Diencephalon-Ppt For BioDocument7 pagesDiencephalon-Ppt For BioLipi UpadhyayNo ratings yet
- Diarrhea: ChildrenDocument16 pagesDiarrhea: ChildrenEmmi Valentina PardedeNo ratings yet
- Fisiologi Manusia: DR Mellova Amir MSCDocument52 pagesFisiologi Manusia: DR Mellova Amir MSCRizal AdhityaNo ratings yet
- Pre AnaestheticsDocument69 pagesPre AnaestheticsPraney SlathiaNo ratings yet
- 10 AsthmaDocument39 pages10 AsthmaAkash MishraNo ratings yet
- The Cardiovascular System: Group 1Document92 pagesThe Cardiovascular System: Group 1Jefferson AdralesNo ratings yet
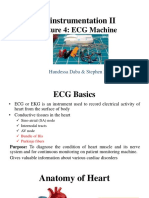
- Bioinstrumentation II: Lecture 4: ECG MachineDocument30 pagesBioinstrumentation II: Lecture 4: ECG MachineHundessa DabaNo ratings yet
- General Anesthetics AbeerDocument45 pagesGeneral Anesthetics AbeerYousef JafarNo ratings yet
- Neurological Assessment PDFDocument52 pagesNeurological Assessment PDFJosephine George JojoNo ratings yet
- Fluid and ElectrolytesDocument137 pagesFluid and ElectrolytesNano Baddour100% (1)
- Drugs in ObstetricsDocument95 pagesDrugs in ObstetricsPriya jNo ratings yet
- Organophosphorus PoisoningDocument14 pagesOrganophosphorus PoisoningSai KrishnaNo ratings yet
- 1 IntroDocument5 pages1 IntroJeanjayannseptoemanNo ratings yet
- 1introDocument158 pages1introDea MaharanisNo ratings yet
- Anatomy and PhysiologyDocument24 pagesAnatomy and PhysiologyGillarhymesNo ratings yet
- OxygenationDocument57 pagesOxygenationassumptaNo ratings yet
- Morphologic Patterns of Acute InflammationDocument51 pagesMorphologic Patterns of Acute Inflammationحفصه حسينNo ratings yet
- Vasodilators: A B C D XDocument1 pageVasodilators: A B C D XPatricia Marie BuenafeNo ratings yet
- Gastrointestinal DrugsDocument2 pagesGastrointestinal DrugsJannah Mikhaela Alibay VillarinNo ratings yet
- Antidiabetic Drug PDFDocument91 pagesAntidiabetic Drug PDFAlifia ainushNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Children's Respiratory NursingFrom EverandChildren's Respiratory NursingJanice MightenNo ratings yet
- Substance Abuse TutorialsDocument3 pagesSubstance Abuse TutorialsjasmingabrielNo ratings yet
- Gateway DrugsDocument6 pagesGateway DrugsMargie Ballesteros ManzanoNo ratings yet
- Modified ASSIST English PDFDocument4 pagesModified ASSIST English PDFRHU MAGSINGALNo ratings yet
- Olanzapine Drug StudyDocument1 pageOlanzapine Drug StudyJeyser T. Gamutia100% (1)
- Upm BenzodiazepinesDocument8 pagesUpm BenzodiazepinesFuad AlamsyahNo ratings yet
- Preventing Drug AbuseDocument176 pagesPreventing Drug AbuseLauraLunguNo ratings yet
- San Angelo ISD - Central Freshman Campus - 2009 Texas School Survey of Drug and Alcohol UseDocument57 pagesSan Angelo ISD - Central Freshman Campus - 2009 Texas School Survey of Drug and Alcohol UseTexas School Survey of Drug and Alcohol UseNo ratings yet
- The Factors of Adolescents To Use Vape at SamarindDocument9 pagesThe Factors of Adolescents To Use Vape at SamarindRobby RanidoNo ratings yet
- Hortatory Exposition TextDocument1 pageHortatory Exposition TextfirasyafriyaniNo ratings yet
- Neuro (Part1) ATIDocument12 pagesNeuro (Part1) ATIGie Lane Ayuyu100% (8)
- Psych 1681444892976Document4 pagesPsych 1681444892976HANNAH BANGKILINGNo ratings yet
- LortabDocument1 pageLortabSheri490No ratings yet
- Canabis Regulacion en Europa-2017 - Cannabistd0217210ennDocument32 pagesCanabis Regulacion en Europa-2017 - Cannabistd0217210enngerardoNo ratings yet
- Unit 5 Pharmacology 1 by ChanduDocument41 pagesUnit 5 Pharmacology 1 by ChanduANAM ARORANo ratings yet
- Obat KosongDocument5 pagesObat KosongMarselina FetraNo ratings yet
- Health 9 2nd Activity 1 Philippine Drug ScenarioDocument2 pagesHealth 9 2nd Activity 1 Philippine Drug ScenarioRyan BersaminNo ratings yet
- AntidepressantDocument8 pagesAntidepressantKlarasita WibowoNo ratings yet
- Anti-Drug Campaigns PolicyReportDocument28 pagesAnti-Drug Campaigns PolicyReportAime Lamoste100% (1)
- MethylphenidateDocument9 pagesMethylphenidateSiegfried CristoforNo ratings yet
- Drug EducationDocument5 pagesDrug EducationChristina Lafayette SesconNo ratings yet
- Inhibitori, Inhibitorii Cresc: Substrat SubstraturileDocument4 pagesInhibitori, Inhibitorii Cresc: Substrat SubstraturileAlina CiugureanuNo ratings yet
- Lawsuit - Tennessee AG Sues Food City For Unlawful Sale of OpioidsDocument209 pagesLawsuit - Tennessee AG Sues Food City For Unlawful Sale of OpioidsDan LehrNo ratings yet
- Laporan Penggunaan Mei 2022Document6 pagesLaporan Penggunaan Mei 2022Rara LaveniaNo ratings yet
- 0812 0819BLDocument15 pages0812 0819BLMelisa AtheyNo ratings yet
- Detailed Lesson Plan in MAPEH Intended in Grade 9 Students Gender and Human Sexuality Integrate With Values EducationDocument6 pagesDetailed Lesson Plan in MAPEH Intended in Grade 9 Students Gender and Human Sexuality Integrate With Values EducationcarNo ratings yet
- 1.) Physical DependenceDocument4 pages1.) Physical DependenceNica Jane SallaoNo ratings yet
- Antipsychotics: Dr. Jai Shri Ram Junior Resident Department of Psychiatry RCSM GMC KolhapurDocument43 pagesAntipsychotics: Dr. Jai Shri Ram Junior Resident Department of Psychiatry RCSM GMC Kolhapurjairamjiki1996No ratings yet