You might also like
- Pipeline Stability and Weight Coating CalculationDocument4 pagesPipeline Stability and Weight Coating CalculationAdaghara67% (3)
- 132kv GISDocument208 pages132kv GISVivek Khedgaonkar100% (5)
- 2018my Zamala BreechmalpresentationDocument72 pages2018my Zamala BreechmalpresentationSaeed HasanNo ratings yet
- Schematic Diagram t240Document6 pagesSchematic Diagram t240dany weinfeldNo ratings yet
- Power Passages and Passenger PDFDocument13 pagesPower Passages and Passenger PDFNestley TiongsonNo ratings yet
- Medical School Companion Obstetrics and Gynecology Practice Question BookFrom EverandMedical School Companion Obstetrics and Gynecology Practice Question BookNo ratings yet
- Cephalopelvic DisproportionDocument5 pagesCephalopelvic DisproportionMaria Donabella OngueNo ratings yet
- BreechDocument38 pagesBreechsanthiyasandy100% (2)
- Shoulder DystociaDocument8 pagesShoulder DystociaMajo MelchiadeNo ratings yet
- BS en 420 2003+a1-2009Document30 pagesBS en 420 2003+a1-2009Abey VettoorNo ratings yet
- Infertilty 2Document9 pagesInfertilty 2Kristine VanzuelaNo ratings yet
- Miscarriages and NutritionDocument70 pagesMiscarriages and NutritionErwin Ginting100% (2)
- Fetal Malpresentations: Abundo, Esther Ellise Espinol, Hazel AnnDocument21 pagesFetal Malpresentations: Abundo, Esther Ellise Espinol, Hazel AnnEsther Ellise Abundo100% (1)
- In Vitro Fertilization: The A.R.T. of Making Babies (Assisted Reproductive Technology)From EverandIn Vitro Fertilization: The A.R.T. of Making Babies (Assisted Reproductive Technology)Rating: 4 out of 5 stars4/5 (1)
- Breech PDFDocument4 pagesBreech PDFMiguel Cuevas Dolot100% (1)
- Well Completion and Stimulation - Chapter 3 Well Performance Analysis-NewDocument56 pagesWell Completion and Stimulation - Chapter 3 Well Performance Analysis-NewsouthliNo ratings yet
- Shoulder PresentationDocument8 pagesShoulder PresentationvincentsharonNo ratings yet
- Threatend AbortionDocument5 pagesThreatend AbortionJohn Walter Torre100% (1)
- Preparing for a Gentle Birth: The Pelvis in PregnancyFrom EverandPreparing for a Gentle Birth: The Pelvis in PregnancyRating: 4 out of 5 stars4/5 (8)
- Fetal Lie Fetal Position: Neither Occiput Nor Sinciput Palpable VaginallyDocument6 pagesFetal Lie Fetal Position: Neither Occiput Nor Sinciput Palpable VaginallyAngelic JoyseNo ratings yet
- OB Dystocia Part II and IIIDocument6 pagesOB Dystocia Part II and IIICyner CruzNo ratings yet
- Factors Affecting Labor.Document2 pagesFactors Affecting Labor.Salman KhanNo ratings yet
- MALPRESENTATIONDocument13 pagesMALPRESENTATIONLady Jane CaguladaNo ratings yet
- Client Initials: Medical Diagnosis: Cephalopelvic Disproportion Eu DEFINITION: The RelationshipDocument2 pagesClient Initials: Medical Diagnosis: Cephalopelvic Disproportion Eu DEFINITION: The RelationshipLyssa Monique67% (3)
- Malpresentations: Liji Raichel Kurian Dept of OBGDocument41 pagesMalpresentations: Liji Raichel Kurian Dept of OBGliji raichel kurian100% (1)
- Adenomyosis PathogenesisDocument18 pagesAdenomyosis Pathogenesisvenkatesh vsNo ratings yet
- rbjQS9 BREECH PRESENTATION-AN OVERVIEWDocument6 pagesrbjQS9 BREECH PRESENTATION-AN OVERVIEWYosita AuroraNo ratings yet
- Antenatal Care 2024 - Student VersionDocument30 pagesAntenatal Care 2024 - Student VersionRoryNo ratings yet
- Etal Osition and ResentationDocument32 pagesEtal Osition and ResentationJennifer Samuel SinghNo ratings yet
- Abnormal Labor, Dystocia IIDocument9 pagesAbnormal Labor, Dystocia IIIke RilleraNo ratings yet
- Articulo 6Document13 pagesArticulo 6Monica ReyesNo ratings yet
- Malpresntation, Malposition and Breech Presentation 2022 BayisaDocument45 pagesMalpresntation, Malposition and Breech Presentation 2022 BayisaHile ShaNo ratings yet
- Uterine Fibroids: Should We Operate?: Stephan Gordts MDDocument47 pagesUterine Fibroids: Should We Operate?: Stephan Gordts MDLizeth Rios ZamoraNo ratings yet
- Module No. Date: Topic:: Cues/Questions/Keywords NotesDocument103 pagesModule No. Date: Topic:: Cues/Questions/Keywords Notesanon ymousNo ratings yet
- Anti IvfDocument18 pagesAnti Ivflyra cosgafaNo ratings yet
- Labor and DeliveryDocument6 pagesLabor and DeliveryHazelGraceNo ratings yet
- 15 Physio OB - Normal LaborDocument8 pages15 Physio OB - Normal LabormaqmmNo ratings yet
- Poster Session I: Study DesignDocument1 pagePoster Session I: Study DesignRegina PizanNo ratings yet
- Labor and Birth Process and NURSING MANAGEMENT (Chapter 13 and 14) False Labor Factors That Affect LaborDocument7 pagesLabor and Birth Process and NURSING MANAGEMENT (Chapter 13 and 14) False Labor Factors That Affect LaborSHARLAIN GAIL V. MELECIONo ratings yet
- Potential Complications Signs and SymptomsDocument2 pagesPotential Complications Signs and SymptomsJessica GomezNo ratings yet
- Legal Med 2.03 Birth, Abortion, InfanticideDocument5 pagesLegal Med 2.03 Birth, Abortion, InfanticideKristine FabellonNo ratings yet
- Ectopic Pregnancy Definition of DisorderDocument48 pagesEctopic Pregnancy Definition of DisorderWRONGHEAR100% (1)
- Multiple PregnancyDocument26 pagesMultiple PregnancyOmar mohamedNo ratings yet
- AmoniakDocument28 pagesAmoniakSulis SipinNo ratings yet
- Abstract:: Abnormal Labor or DystociaDocument3 pagesAbstract:: Abnormal Labor or DystociawidyaNo ratings yet
- Increased Fetal Weight Problems With The Fetal Position/ Attitude Problems With The Pelvis Problems With The Genital TractDocument1 pageIncreased Fetal Weight Problems With The Fetal Position/ Attitude Problems With The Pelvis Problems With The Genital TractCarlo Joseph Intal LlacerNo ratings yet
- Breech PresentationDocument85 pagesBreech Presentationwidya vannesaNo ratings yet
- 556 - Breechwilliams Obstetrics 25th Edition (2018)Document12 pages556 - Breechwilliams Obstetrics 25th Edition (2018)yayayanizaNo ratings yet
- Slides Mullerian AnomaliesDocument29 pagesSlides Mullerian AnomaliesAsunción AncoNo ratings yet
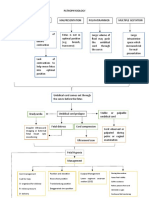
- Pathophysio (Ucp)Document2 pagesPathophysio (Ucp)Rachelle Joy AsuncionNo ratings yet
- 10 1371@journal Pone 0225546Document13 pages10 1371@journal Pone 0225546Karina AzaleaNo ratings yet
- Definition: Related Diagnostic TestsDocument8 pagesDefinition: Related Diagnostic TestsQuinn Xylon VillanuevaNo ratings yet
- Maternal Movement For Better OutcomesDocument36 pagesMaternal Movement For Better OutcomesliverpooldoulaNo ratings yet
- Case Reflection 1 POD 1Document7 pagesCase Reflection 1 POD 1seankelly327No ratings yet
- What Can The Clinician Do To Improve Implantation?: OutlookDocument11 pagesWhat Can The Clinician Do To Improve Implantation?: OutlookGayathriMaranNo ratings yet
- JUWAK, JASSIM - Act 1Document5 pagesJUWAK, JASSIM - Act 1JASSIM JUWAKNo ratings yet
- Predictors of Cephalopelvic Disproportion in Labour A Tertiary Hospital in Bayelsa State, NigeriaDocument7 pagesPredictors of Cephalopelvic Disproportion in Labour A Tertiary Hospital in Bayelsa State, NigeriaAndri Muhrim SiddiqNo ratings yet
- Breechpresentation Copy 141124075623 Conversion Gate02 PDFDocument38 pagesBreechpresentation Copy 141124075623 Conversion Gate02 PDFKathirNo ratings yet
- Rupture Uterus in Pregnancy With Didelphys Uterus: A Rare Case ReportDocument3 pagesRupture Uterus in Pregnancy With Didelphys Uterus: A Rare Case Reportanon_804324181No ratings yet
- Malpositions and Malpresentations of The Fetal Head: ReviewDocument9 pagesMalpositions and Malpresentations of The Fetal Head: ReviewIntan PermataNo ratings yet
- Poster Session I: Results: Study DesignDocument2 pagesPoster Session I: Results: Study DesignFatih AkbarNo ratings yet
- Breech PresentationDocument2 pagesBreech PresentationDiane Angelique ArceoNo ratings yet
- Respiratory Consequences of Preterm BirthDocument5 pagesRespiratory Consequences of Preterm BirthAidillahMayudaNo ratings yet
- Selecting Male Or Female Child Here's How It Works - Based On The Teachings Of Dr. Andrew Huberman: A Guide To Gender SelectionFrom EverandSelecting Male Or Female Child Here's How It Works - Based On The Teachings Of Dr. Andrew Huberman: A Guide To Gender SelectionNo ratings yet
- FINAL LIST OF JOB ROLES FOR PMKVY 2 (Release Date 26-08-16)Document8 pagesFINAL LIST OF JOB ROLES FOR PMKVY 2 (Release Date 26-08-16)udi969No ratings yet
- Quicklink Networks Janitor Imbs 2.0 2Document1 pageQuicklink Networks Janitor Imbs 2.0 2Vrujesh BhattNo ratings yet
- Microwave DiathermyDocument4 pagesMicrowave DiathermyDragan CvetkovicNo ratings yet
- Phillip Island: UnderstandDocument3 pagesPhillip Island: UnderstandMeiyappan MuniandyNo ratings yet
- (Journal of NeurosurgeDocument10 pages(Journal of NeurosurgeMoustafa FouadNo ratings yet
- Lahiry 2021Document11 pagesLahiry 2021AsmaNo ratings yet
- Week 2 Branches of SocologyDocument15 pagesWeek 2 Branches of SocologyLaiba MunirNo ratings yet
- Advanced Enzymes Acquires 70% Stake in API Maker JC Biotech (Company Update)Document2 pagesAdvanced Enzymes Acquires 70% Stake in API Maker JC Biotech (Company Update)Shyam SunderNo ratings yet
- Assessment Task 1: Knowledge TestDocument38 pagesAssessment Task 1: Knowledge TestSukhin ChauhanNo ratings yet
- Sanctorom of Goddess Padmavathi EnglishDocument85 pagesSanctorom of Goddess Padmavathi EnglishsanathandharmaNo ratings yet
- Oxides of Nitrogen FINALDocument20 pagesOxides of Nitrogen FINALBin RenNo ratings yet
- Energy IsolamentoDocument24 pagesEnergy IsolamentoArtur KinalNo ratings yet
- Practice Test 1: Doan Thi Diem Secondary SchoolDocument10 pagesPractice Test 1: Doan Thi Diem Secondary SchoolMai Hà AnhNo ratings yet
- Advocacy and Sustainable Development in NigeriaDocument5 pagesAdvocacy and Sustainable Development in Nigeriavinay kumarNo ratings yet
- Dairy IndustryDocument11 pagesDairy IndustryAbhishek SharmaNo ratings yet
- API 5L Pipes For Pipelines Explained - ProjectmaterialsDocument21 pagesAPI 5L Pipes For Pipelines Explained - ProjectmaterialsMehrshad ShakibNo ratings yet
- 2009-07-04 170949 Mazda TimingDocument8 pages2009-07-04 170949 Mazda TimingSuksan SananmuangNo ratings yet
- Sachin Sharma ProfileDocument45 pagesSachin Sharma ProfileSandip PurohitNo ratings yet
- Hangcha 10TNDocument2 pagesHangcha 10TNFreddy AndresNo ratings yet
- The Opportunity: Measurement of Furnace Exit-Gas Temperature (Fegt)Document4 pagesThe Opportunity: Measurement of Furnace Exit-Gas Temperature (Fegt)muhdmsohNo ratings yet
- Faculty of Engineering and The Built EnvironmentDocument5 pagesFaculty of Engineering and The Built EnvironmentPrecious Fufu MkhontoNo ratings yet
- YoonA - Jung Siwoos A Room InterviewDocument13 pagesYoonA - Jung Siwoos A Room Interviewchuachua.deNo ratings yet
- 2022 Recycled Non-Biodegradable Polyethylene Terephthalate Waste As Fine Aggregate in Fly Ash Geopolymer and Cement MortarsDocument12 pages2022 Recycled Non-Biodegradable Polyethylene Terephthalate Waste As Fine Aggregate in Fly Ash Geopolymer and Cement MortarsAbdelrahman AshmawyNo ratings yet
- OD2e L5 Tests Unit 2Document2 pagesOD2e L5 Tests Unit 2gilbert silva0% (1)