You might also like
- Menilai Jurnal (CAT)Document53 pagesMenilai Jurnal (CAT)Risya TheupstarNo ratings yet
- Checklist RCTDocument5 pagesChecklist RCTFajar SukmajayaNo ratings yet
- Critical Appraisal: Prof. Dr. Mohammad Hakimi, Spog (K), PHDDocument37 pagesCritical Appraisal: Prof. Dr. Mohammad Hakimi, Spog (K), PHDFebbty KuswantiNo ratings yet
- K7 - Critical AppraisalDocument40 pagesK7 - Critical AppraisalFiqih IbrahimNo ratings yet
- Evidence-Based Medicine in Clinical PracticeDocument42 pagesEvidence-Based Medicine in Clinical PracticeNur Rahmah KurniantiNo ratings yet
- EBM Worksheets (Therapy, Diagnosis, Prognosis, Economic, Guideline, Decision Making)Document15 pagesEBM Worksheets (Therapy, Diagnosis, Prognosis, Economic, Guideline, Decision Making)Soffatul AzizahNo ratings yet
- Evidence Based Medicine and Practice: Critical Appraisal of Prognostic StudiesDocument2 pagesEvidence Based Medicine and Practice: Critical Appraisal of Prognostic StudiesMuhammad BilalNo ratings yet
- Critical Appraisal WorksheetsDocument10 pagesCritical Appraisal WorksheetsHotmann XtinusNo ratings yet
- Ebm&Rm Dta Student 2023Document14 pagesEbm&Rm Dta Student 2023Sara Abdi OsmanNo ratings yet
- Harm Wsheet Revise Cohort Case CTRLDocument4 pagesHarm Wsheet Revise Cohort Case CTRL54. Alfredo Abrian Erlangga SetiawanNo ratings yet
- Critical appraisal of journal articles: A guide to evaluating research evidenceDocument29 pagesCritical appraisal of journal articles: A guide to evaluating research evidencemonique marwick100% (2)
- Critical Appraisal 2017Document65 pagesCritical Appraisal 2017Fransiscus RivaldyNo ratings yet
- Critical Appraisal Checklist For An Article OnDocument4 pagesCritical Appraisal Checklist For An Article OnTiaz DiniutamiNo ratings yet
- Critical Appraisal of Cohort Studies EBMP 1000e108Document2 pagesCritical Appraisal of Cohort Studies EBMP 1000e108thetaggerung100% (1)
- Critical Appraisal Checklist For An Article On Treatment or PreventionDocument4 pagesCritical Appraisal Checklist For An Article On Treatment or PreventionSaina AbasNo ratings yet
- Critical Appraisal Checklist For An Article On Decision AnalysisDocument4 pagesCritical Appraisal Checklist For An Article On Decision AnalysisT.a. TemesgenNo ratings yet
- Evidence Based Mecidine (Ebm) : Laporan PraktikumDocument6 pagesEvidence Based Mecidine (Ebm) : Laporan Praktikumlailatut toriqohNo ratings yet
- Evidence-Based Medicine MamanDocument79 pagesEvidence-Based Medicine MamanAlma WijayaNo ratings yet
- JC Presentation FormatDocument12 pagesJC Presentation FormatNikitha AshokNo ratings yet
- Diy RCT AppraisalDocument43 pagesDiy RCT AppraisalimperiallightNo ratings yet
- An Introduction To Critical Appraisal: Training NotesDocument12 pagesAn Introduction To Critical Appraisal: Training NotesRima ZahraNo ratings yet
- Critical Appraisal CriteriaDocument3 pagesCritical Appraisal CriteriaputrivbpNo ratings yet
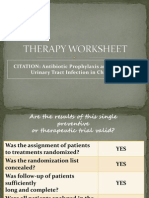
- CITATION: Antibiotic Prophylaxis and Recurrent Urinary Tract Infection in ChildrenDocument16 pagesCITATION: Antibiotic Prophylaxis and Recurrent Urinary Tract Infection in Childrenchristian_friztNo ratings yet
- Journal Club FormatDocument3 pagesJournal Club Formatylliafwn100% (1)
- EBP Presentation by Group 2Document25 pagesEBP Presentation by Group 2Dr-Muhammad QasimNo ratings yet
- Critical Appraisal For RCT & Meta AnalisisDocument8 pagesCritical Appraisal For RCT & Meta AnalisisHanniNo ratings yet
- Critical AppraisalDocument6 pagesCritical AppraisalRevina AmaliaNo ratings yet
- Critical Appraisal The ApplicabilityDocument32 pagesCritical Appraisal The ApplicabilityTalha Basharat AliNo ratings yet
- THERAPYDocument58 pagesTHERAPYjuwitutNo ratings yet
- Critical Appraisal ChecklistDocument9 pagesCritical Appraisal Checklisttias nurainiNo ratings yet
- Critically Appraised Topics 23june2014Document33 pagesCritically Appraised Topics 23june2014filchibuffNo ratings yet
- Evidence-Based Medicine Therapy: Dr. Dr. Rina Amelia, MARS Departemen Kedokteran Komunitas FK USUDocument40 pagesEvidence-Based Medicine Therapy: Dr. Dr. Rina Amelia, MARS Departemen Kedokteran Komunitas FK USUSamuel TanNo ratings yet
- Therapy Worksheet 2Document1 pageTherapy Worksheet 2stylesh828No ratings yet
- Critical Appraisal - Therapy - APTDocument36 pagesCritical Appraisal - Therapy - APTJason LiberiNo ratings yet
- Evidence Based Ophthalmology: Noel D. Atienza, MD, MSCDocument59 pagesEvidence Based Ophthalmology: Noel D. Atienza, MD, MSCJanBarlaanNo ratings yet
- MEDECIELO MELO - Chapter 8 SummaryDocument7 pagesMEDECIELO MELO - Chapter 8 SummaryMelo MedecieloNo ratings yet
- Critical Appraisal JRDocument3 pagesCritical Appraisal JRRizky AgustriaNo ratings yet
- EBM Presentation SummaryDocument23 pagesEBM Presentation SummaryTejus Murthy A G100% (2)
- Critical Appraisal Guide: Research MethodologyDocument3 pagesCritical Appraisal Guide: Research MethodologylizNo ratings yet
- CriticalAppraisalWorksheetTherapy EffectSizeDocument2 pagesCriticalAppraisalWorksheetTherapy EffectSizeFitriArdiningsihNo ratings yet
- Therapy Worksheet Title of Article: Authors: Journal: BackgroundDocument3 pagesTherapy Worksheet Title of Article: Authors: Journal: BackgroundRandi Kosim SiregarNo ratings yet
- EBM - Therapy: Gita Sekar PrihantiDocument116 pagesEBM - Therapy: Gita Sekar PrihantiMuhammida Fahriana100% (1)
- Protokol Critical ApraisalDocument16 pagesProtokol Critical ApraisalMustika ayu lestariNo ratings yet
- Best Practice & Research Clinical RheumatologyDocument13 pagesBest Practice & Research Clinical RheumatologydrharivadanNo ratings yet
- Template Critical AppraisalDocument9 pagesTemplate Critical AppraisalFarhana AmaliyahNo ratings yet
- AD 8 Journal Eng VersionDocument30 pagesAD 8 Journal Eng VersionGamer MadaNo ratings yet
- Aetiology or Harm Critical Appraisal Guide: ValidityDocument3 pagesAetiology or Harm Critical Appraisal Guide: ValidityMELLY RAHMAWATINo ratings yet
- Analisis RCT Continuous Outcome - Google SearchDocument13 pagesAnalisis RCT Continuous Outcome - Google SearchRaudhatulAisyFachrudinNo ratings yet
- Experimental RCT StudiesDocument35 pagesExperimental RCT StudiesLusungu S. LupenzaNo ratings yet
- Reviewing a Decision AnalysisDocument13 pagesReviewing a Decision AnalysisKevin Mora BañosNo ratings yet
- Introduction Should Clearly State The Question. If YouDocument4 pagesIntroduction Should Clearly State The Question. If Youandri kurniaNo ratings yet
- Evidence Based Medicine Series: Part 3. Appraising The Evidence Are The Results Valid and Clinically Important?Document6 pagesEvidence Based Medicine Series: Part 3. Appraising The Evidence Are The Results Valid and Clinically Important?Ice Bear JJNo ratings yet
- EBCR Refreshing For ResidentsDocument47 pagesEBCR Refreshing For ResidentsJohn Patria Maruli SinagaNo ratings yet
- "Evidence-Based Medicine" TherapyDocument54 pages"Evidence-Based Medicine" TherapyRuthra Devi NarayanasamyNo ratings yet
- Evidence-Based Medicine in PRACTICEDocument63 pagesEvidence-Based Medicine in PRACTICEAppu JhaNo ratings yet
- 4 20190629 Detty Cochrane Indonesia UGM Champion Systematic ReviewDocument87 pages4 20190629 Detty Cochrane Indonesia UGM Champion Systematic ReviewRafaela LennyNo ratings yet
- Estimation of The Quality of Pre-Operative Anesthesia Evaluation PracticeDocument9 pagesEstimation of The Quality of Pre-Operative Anesthesia Evaluation PracticeHassan Shuaaieb Mohamed ShaaibNo ratings yet
- Diagnostic Test Bias Risk AssessmentDocument1 pageDiagnostic Test Bias Risk AssessmentDewi SriNo ratings yet
- Evidence Based Practice: Ilham, Ners, M. KepDocument17 pagesEvidence Based Practice: Ilham, Ners, M. KepBaiq ItaNo ratings yet
- Adrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing SyndromeDocument46 pagesAdrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing Syndromeyuyu tuptupNo ratings yet
- Reproductive Tests in FemalesDocument33 pagesReproductive Tests in Femalesyuyu tuptupNo ratings yet
- Thyroid Gland: Ruswana Anwar, Tono DjuwantonoDocument49 pagesThyroid Gland: Ruswana Anwar, Tono Djuwantonoyuyu tuptupNo ratings yet
- NeuroendocrinologyDocument58 pagesNeuroendocrinologyyuyu tuptupNo ratings yet
- Meta Analysis: Ruswana Anwar, Herman WibisonoDocument25 pagesMeta Analysis: Ruswana Anwar, Herman Wibisonoyuyu tuptup100% (1)
- Developmental Genetics and EmbryogenesisDocument18 pagesDevelopmental Genetics and Embryogenesisyuyu tuptupNo ratings yet
- Treatment of Genetic Diseases Through Symptomatic Relief, Metabolic Correction, and Gene TherapyDocument23 pagesTreatment of Genetic Diseases Through Symptomatic Relief, Metabolic Correction, and Gene Therapyyuyu tuptupNo ratings yet
- Genetics and Environmental InteractionDocument11 pagesGenetics and Environmental Interactionyuyu tuptupNo ratings yet
- Dna, Replikasi, Transkripsi Dan Translasi DR - Ruswana Anwar, Spog Pembimbing DR - Herman Wibisono MS, SpandDocument41 pagesDna, Replikasi, Transkripsi Dan Translasi DR - Ruswana Anwar, Spog Pembimbing DR - Herman Wibisono MS, Spandyuyu tuptupNo ratings yet
- Konsep Dasar Imunologi: DR Ruswana Anwar Spog Pembimbing: DR Tita Husnitawati MajidspogDocument42 pagesKonsep Dasar Imunologi: DR Ruswana Anwar Spog Pembimbing: DR Tita Husnitawati Majidspogyuyu tuptupNo ratings yet
- Thyroid Gland: Ruswana Anwar, Tono DjuwantonoDocument49 pagesThyroid Gland: Ruswana Anwar, Tono Djuwantonoyuyu tuptupNo ratings yet
- Genetika DasarDocument23 pagesGenetika Dasaryuyu tuptupNo ratings yet
- Endometriosis: Aetiology, Pathogenesis and TreatmentDocument16 pagesEndometriosis: Aetiology, Pathogenesis and Treatmentyuyu tuptupNo ratings yet
- Kuliah Endocrinology of PregnancyDocument2 pagesKuliah Endocrinology of Pregnancyyuyu tuptupNo ratings yet
- Tayangan Immunologi DR AgusDocument29 pagesTayangan Immunologi DR Agusyuyu tuptupNo ratings yet
- Hirschsprung Disease ExplainedDocument14 pagesHirschsprung Disease Explainedyuyu tuptupNo ratings yet
- 2012 Infant Mortality ReportDocument52 pages2012 Infant Mortality ReportSusie CambriaNo ratings yet
- Umbilical Cord ProlapseDocument26 pagesUmbilical Cord Prolapsesulekhaanoob100% (2)
- ComaDocument13 pagesComaMamoon J. MehdiNo ratings yet
- Aden Abdi-ResumeDocument2 pagesAden Abdi-Resumeapi-534490436No ratings yet
- Prinsip Kedokteran Keluarga 2018Document57 pagesPrinsip Kedokteran Keluarga 2018BisukNo ratings yet
- Antibiotic ChartsDocument61 pagesAntibiotic Chartspempekplg100% (1)
- Check Your English Vocabulary For MedicineDocument65 pagesCheck Your English Vocabulary For MedicineOlga Poleszak100% (1)
- P7b11toc Gastroenterology and NutritionDocument19 pagesP7b11toc Gastroenterology and NutritionWidya Lestari CapawatyNo ratings yet
- BARANGAY MONTHLY INVENTORY OF VACCINATED POPULATIONDocument108 pagesBARANGAY MONTHLY INVENTORY OF VACCINATED POPULATIONAna Marie BergoniaNo ratings yet
- British Orthoptic Journal 2002Document9 pagesBritish Orthoptic Journal 2002roelkloosNo ratings yet
- HydramniosDocument31 pagesHydramniosSpandana DepuruNo ratings yet
- 1 s2.0 S0828282X22001271 MainDocument11 pages1 s2.0 S0828282X22001271 MainLilianne Mbengani LaranjeiraNo ratings yet
- Supracondylar Fractures of The Humerus in Children Review of Management and Controversies 2161 0533 1000206 PDFDocument8 pagesSupracondylar Fractures of The Humerus in Children Review of Management and Controversies 2161 0533 1000206 PDFAlvin GfNo ratings yet
- The International Workshop On Meibomian GlandDocument44 pagesThe International Workshop On Meibomian GlandPutri kartiniNo ratings yet
- Central Nervous System MedicationsDocument12 pagesCentral Nervous System MedicationsMARY JEANINA ALBANo ratings yet
- 4 Sedation Care PolicyDocument5 pages4 Sedation Care PolicyFarah Andleeb MalikNo ratings yet
- Triphala in Endodontics-A ReviewDocument5 pagesTriphala in Endodontics-A ReviewBOHR International Journal of Current research in Dentistry (BIJCRID)No ratings yet
- BB Pheresis GuidelinesDocument190 pagesBB Pheresis GuidelinesBill ThomNo ratings yet
- DSM 5 Diagnostic CategoriesDocument15 pagesDSM 5 Diagnostic Categoriesmomo connor100% (2)
- ResearchDocument6 pagesResearchhaerul ikhsanNo ratings yet
- Stem List CumulativeDocument34 pagesStem List Cumulativeleesteph78No ratings yet
- Health6 - q1 - Mod5 - Identifies Community Health Resources and Facilities - FINAL.Document24 pagesHealth6 - q1 - Mod5 - Identifies Community Health Resources and Facilities - FINAL.vamps sier100% (1)
- b7 PPT, AntihistaminesDocument56 pagesb7 PPT, AntihistaminesKeziah GillNo ratings yet
- LabCorp provides age-specific pediatric reference rangesDocument14 pagesLabCorp provides age-specific pediatric reference rangesshoratanNo ratings yet
- Pregnancy Induced Hypertension (Pih)Document56 pagesPregnancy Induced Hypertension (Pih)shandi23100% (5)
- Case Stydy Angina PectorisDocument46 pagesCase Stydy Angina PectorissharenNo ratings yet
- Tuberculosis of Bones and JointsDocument19 pagesTuberculosis of Bones and JointsreinNo ratings yet
- Physical Exercise and PsychologicalDocument10 pagesPhysical Exercise and Psychologicalbodeadumitru9261100% (1)
- Onclolgy in AyurvedaDocument10 pagesOnclolgy in AyurvedaYoga FMUNo ratings yet
- NonCytotoxic Dibenzyl and Also Difluoroborate Capmatinibxlsxoid Fluorophores Permit Visual Image Involving Nucleus or Even Cytoplasm Inside Bioimagingixvwj PDFDocument1 pageNonCytotoxic Dibenzyl and Also Difluoroborate Capmatinibxlsxoid Fluorophores Permit Visual Image Involving Nucleus or Even Cytoplasm Inside Bioimagingixvwj PDFtubweed4No ratings yet