You might also like
- Acute Renal FailureDocument25 pagesAcute Renal FailureRyan Akhmad Adhi SaputraNo ratings yet
- Human Body Systems Chart With Pictures Answers-Option ADocument3 pagesHuman Body Systems Chart With Pictures Answers-Option AJamie Sims100% (2)
- Nephrology For Medical StudentsDocument20 pagesNephrology For Medical StudentsAhmed El AlfyNo ratings yet
- 3f Aubf Lec Renal Function Tests PDFDocument11 pages3f Aubf Lec Renal Function Tests PDFBanana QNo ratings yet
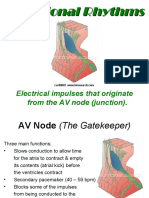
- Irama JunctionalDocument18 pagesIrama JunctionalTaufik Nur YahyaNo ratings yet
- Handbook On Spa and Massage 4 X 6 DraftDocument44 pagesHandbook On Spa and Massage 4 X 6 DraftBenjie EugenioNo ratings yet
- Penyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUDocument56 pagesPenyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUFitriana WijayatiNo ratings yet
- TiroidDocument26 pagesTiroidJoni Riana MustaqimNo ratings yet
- Master Radiology Notes UrologyDocument106 pagesMaster Radiology Notes UrologySafwan ShaikhNo ratings yet
- Acute Kidney InjuryDocument16 pagesAcute Kidney InjuryPutrii Rahayu Sriikandi100% (1)
- Kuliah 16 Cor PulmonaleDocument41 pagesKuliah 16 Cor PulmonalecaturwiraNo ratings yet
- Gagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanDocument20 pagesGagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanAdlan BinharyantoNo ratings yet
- A Critical Study On Boenninghausens Therapeutic Pocket BookDocument10 pagesA Critical Study On Boenninghausens Therapeutic Pocket BookamblingbyNo ratings yet
- Gasem MH HANTA Salatiga 2019Document43 pagesGasem MH HANTA Salatiga 2019ChristianNo ratings yet
- Icd XDocument3 pagesIcd XR Ghianesya GantinaNo ratings yet
- 2016 PAD ACC+AHA SlidesDocument74 pages2016 PAD ACC+AHA SlidesPonpimol Odee BongkeawNo ratings yet
- Clinical Aspects of PneumothoraxDocument3 pagesClinical Aspects of PneumothoraxelisabethNo ratings yet
- Chronic Liver DiseaseDocument3 pagesChronic Liver DiseaseMohammad AbbasNo ratings yet
- Pancreatic MalignancyDocument22 pagesPancreatic Malignancylovelots1234No ratings yet
- Prof. Syakib Acute Kidney Injury - Internal Medicine Emergency Course - Agustus 2019-DikonversiDocument35 pagesProf. Syakib Acute Kidney Injury - Internal Medicine Emergency Course - Agustus 2019-DikonversidrroytambunanNo ratings yet
- OsteomielitisDocument28 pagesOsteomielitismaulidaangraini100% (1)
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- HSP and ITPDocument2 pagesHSP and ITPSara Vowels-Hattaway100% (3)
- AKI & Indikasi CRRTDocument25 pagesAKI & Indikasi CRRTMaya Sari BaharumNo ratings yet
- Lutembacher's Syndrome at KolonodaleDocument7 pagesLutembacher's Syndrome at KolonodaleWayan GunawanNo ratings yet
- PansitopeniaDocument33 pagesPansitopeniaBrad WrightNo ratings yet
- Overview of The Mucopolysaccharidoses: RheumatologyDocument9 pagesOverview of The Mucopolysaccharidoses: RheumatologyLaura Orjuela MateusNo ratings yet
- Episkleritis N Skleritis EditDocument12 pagesEpiskleritis N Skleritis EditAnonymous HgX3mN1oNo ratings yet
- Bilas LambungDocument12 pagesBilas LambungNthie UnguNo ratings yet
- Referat Malaria SerebralDocument42 pagesReferat Malaria SerebralLivia HanisamurtiNo ratings yet
- Sindrom NefrotikDocument22 pagesSindrom NefrotikGyta Apriati100% (1)
- Diabeticum Ketoacidosis: Ach. Najich RF, DRDocument16 pagesDiabeticum Ketoacidosis: Ach. Najich RF, DRAch Najich RfNo ratings yet
- Patch Test ROAT PDFDocument9 pagesPatch Test ROAT PDFrochmandrg dokter gigiNo ratings yet
- Interpretasi Hasil Analisa Gas Darah: (Formula Anderson-Hasselbach)Document28 pagesInterpretasi Hasil Analisa Gas Darah: (Formula Anderson-Hasselbach)mafoel39No ratings yet
- Acs OsceDocument4 pagesAcs OsceYohanes ArviNo ratings yet
- RozerplastyDocument4 pagesRozerplastyLutfi Aulia RahmanNo ratings yet
- Kul Sem 4 Heat Stroke N Fever UHT 2016Document63 pagesKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaNo ratings yet
- n378.008 Iris Website Staging of CKD PDFDocument8 pagesn378.008 Iris Website Staging of CKD PDFrutebeufNo ratings yet
- Tonsillitis Diphteri: Literature ReadingDocument28 pagesTonsillitis Diphteri: Literature ReadingFebryantiPBundaayabariq100% (1)
- Anemia Def B12 Dan As FolatDocument30 pagesAnemia Def B12 Dan As Folatinas khoirunnisaNo ratings yet
- 194 Surgical Cases PDFDocument160 pages194 Surgical Cases PDFkint100% (4)
- 2 DHF InternaDocument59 pages2 DHF Internasaladass 2No ratings yet
- KARDIOMYOPATI - Kuliah DR - ErlinaDocument28 pagesKARDIOMYOPATI - Kuliah DR - ErlinaArif Zulfian MubarokNo ratings yet
- Update Management of Acute StrokeDocument48 pagesUpdate Management of Acute StrokerintyosoNo ratings yet
- BrucellosisDocument26 pagesBrucellosisVasilika GiemsaNo ratings yet
- LPRDocument30 pagesLPRLiza HutahaeanNo ratings yet
- Refreshing DHFDocument13 pagesRefreshing DHFNia Nurhayati ZakiahNo ratings yet
- HDDocument23 pagesHDSardjitoNo ratings yet
- REFERAT Cluster HeadacheDocument39 pagesREFERAT Cluster HeadacheSafitriNo ratings yet
- Hipertiroid HarrisonDocument8 pagesHipertiroid HarrisonravenskaNo ratings yet
- Geriatric Medicine KuliahDocument38 pagesGeriatric Medicine KuliahLia pramitaNo ratings yet
- Pemasangan Dan Interpretasi EKGDocument117 pagesPemasangan Dan Interpretasi EKGaulianadanisya100% (2)
- CR Piopneumothoraks Nicky FIXdDocument62 pagesCR Piopneumothoraks Nicky FIXdPutri RahmawatiNo ratings yet
- Asthma + COPD - 2022 LectureDocument85 pagesAsthma + COPD - 2022 Lecturedesti purnama sariNo ratings yet
- Soft Tissue TumorDocument248 pagesSoft Tissue TumorDabessa MosissaNo ratings yet
- Dr. Uun Sumardi, SPPD, K-PTI, KIC, FINASIM-Fluid Management in Severe DengueDocument20 pagesDr. Uun Sumardi, SPPD, K-PTI, KIC, FINASIM-Fluid Management in Severe DengueOlivia DwimaswastiNo ratings yet
- Blighted OvumDocument31 pagesBlighted OvumHeri FarnasNo ratings yet
- Albumin in Liver Cirrhosis, SADocument37 pagesAlbumin in Liver Cirrhosis, SADwinita ViviantiNo ratings yet
- Journal Reading THT - OMADocument15 pagesJournal Reading THT - OMAIndira MaycellaNo ratings yet
- Leptospirosis by DR SarmaDocument37 pagesLeptospirosis by DR SarmaTias Diah0% (1)
- Daftar Kode Diagnosa & TindakanDocument7 pagesDaftar Kode Diagnosa & Tindakannovi andriyaniNo ratings yet
- Kegawatan Respirasi May2016-FkumyDocument62 pagesKegawatan Respirasi May2016-FkumyAgustina Tri P. DNo ratings yet
- Batu Saluran Kemih: Dr. Suhaemi, SPPD, FinasimDocument57 pagesBatu Saluran Kemih: Dr. Suhaemi, SPPD, FinasimAfri AdiNo ratings yet
- Jurding PVDocument17 pagesJurding PVAnisaAyuningtyasNo ratings yet
- Askep MCI - AchirmanDocument53 pagesAskep MCI - AchirmanmarthaNo ratings yet
- TUGAS IPD 1-50 + DapusDocument17 pagesTUGAS IPD 1-50 + DapusM. RamazaliNo ratings yet
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisFrom EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisRating: 3.5 out of 5 stars3.5/5 (2)
- Glo Me Rulo NefritisDocument58 pagesGlo Me Rulo NefritisFany SholehaNo ratings yet
- Renal Glycosuria Case StudyDocument2 pagesRenal Glycosuria Case StudyRodeoKenan100% (1)
- Learn CBSE: MCQ Questions For Class 10 Science Life Process With AnswersDocument8 pagesLearn CBSE: MCQ Questions For Class 10 Science Life Process With AnswersAbu-mu'aadh Abdulqaadr Bn AdebayoNo ratings yet
- Zinner's Syndrome: A New Asymptomatic Case ReportDocument3 pagesZinner's Syndrome: A New Asymptomatic Case ReportasclepiuspdfsNo ratings yet
- Dr. YeshwiniDocument34 pagesDr. YeshwiniSai RakshikaNo ratings yet
- Uroradiology Tutorial For Medical StudentsDocument65 pagesUroradiology Tutorial For Medical StudentsmerikasorNo ratings yet
- Disorders of Urinary Tract - NewDocument4 pagesDisorders of Urinary Tract - NewshshanksNo ratings yet
- Casts in UrineDocument64 pagesCasts in UrineNitin Rathod100% (1)
- 057 Pathology MCQ ACEM Primary RenalDocument5 pages057 Pathology MCQ ACEM Primary RenalStarlightNo ratings yet
- 7 Urinary Disorders - 2012 - Small Animal Clinical Diagnosis by Laboratory Methods Fifth EditionDocument30 pages7 Urinary Disorders - 2012 - Small Animal Clinical Diagnosis by Laboratory Methods Fifth EditionNarvarte Hospital Veterinario de EspecialidadesNo ratings yet
- Lecture (5) Kidney Function Tests Part IDocument33 pagesLecture (5) Kidney Function Tests Part IAmine GobranNo ratings yet
- Nephrotic Syndrome - Armando HasudunganDocument18 pagesNephrotic Syndrome - Armando HasudunganzahraaNo ratings yet
- Apeejay Stya University: Diploma in Pharmacy (D.Pharm.) June 2018 COURSE STRUCTURE - Human Anatomy & PhysiologyDocument5 pagesApeejay Stya University: Diploma in Pharmacy (D.Pharm.) June 2018 COURSE STRUCTURE - Human Anatomy & PhysiologyPoonam VermaNo ratings yet
- Renal SystemDocument18 pagesRenal SystemS GNo ratings yet
- NephrolithiasisDocument3 pagesNephrolithiasisVince GagarNo ratings yet
- Renal Acute Kidney InjuryDocument41 pagesRenal Acute Kidney InjuryTim SilvaNo ratings yet
- AHS 101 Anatomy and Physiology SyllabusDocument14 pagesAHS 101 Anatomy and Physiology SyllabusJuan ConcepcionNo ratings yet
- 2 UrinarySystemDocument83 pages2 UrinarySystemLemuel Lagasca Razalan IVNo ratings yet
- Mehu108 - U4 - T6 - Cáncer Urológico 2Document22 pagesMehu108 - U4 - T6 - Cáncer Urológico 2Jose Jared Sernaque NavarroNo ratings yet
- CombinedDocument97 pagesCombinedEswara PrasadNo ratings yet
- IgA NephrophathyDocument4 pagesIgA NephrophathyyousifNo ratings yet
- Urinary Tract InfectionsDocument35 pagesUrinary Tract InfectionsCharity Grace Magno100% (1)
- Bimbingan IMO UroreproDocument12 pagesBimbingan IMO UroreproFatimah AzzahraNo ratings yet