You might also like
- Appearances of Human Milk Bright Yellow ColostrumDocument28 pagesAppearances of Human Milk Bright Yellow Colostrumjaish8904100% (3)
- OB-Gyn Case Presentation - BicornuateDocument53 pagesOB-Gyn Case Presentation - BicornuateZari Novela100% (1)
- The Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachDocument8 pagesThe Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachqisthiaufaNo ratings yet
- Supports of The UterusDocument20 pagesSupports of The UterusAshwin Prem Solomon100% (1)
- SGOP 2008 (Guidelines On Management)Document87 pagesSGOP 2008 (Guidelines On Management)Via Alip100% (1)
- Approach To The Patient With An Adnexal Mass - UpToDateDocument31 pagesApproach To The Patient With An Adnexal Mass - UpToDateRamackNo ratings yet
- Fibroid Uterus 2019Document60 pagesFibroid Uterus 2019Mahmoud Abu Al AmrainNo ratings yet
- Abnormal Uterine BleedingDocument39 pagesAbnormal Uterine BleedingVincentiusNo ratings yet
- PA Genitalia WanitaDocument100 pagesPA Genitalia WanitaBNo ratings yet
- Sakila MurmuDocument47 pagesSakila MurmuSakila murmuNo ratings yet
- Cornual Ectopic PregnancyDocument1 pageCornual Ectopic PregnancyPavani NallaluthanNo ratings yet
- Malignant Tumors of Uterus: DR Tahira RizwanDocument52 pagesMalignant Tumors of Uterus: DR Tahira RizwanSadia YousafNo ratings yet
- Malaria in PregnancyDocument9 pagesMalaria in Pregnancyamarendra WardhanaNo ratings yet
- Uterinefibroids 130120064643 Phpapp02Document73 pagesUterinefibroids 130120064643 Phpapp02Tharun KumarNo ratings yet
- Understanding Uterine FibroidsDocument52 pagesUnderstanding Uterine FibroidsDoctor JitNo ratings yet
- Uterine FibroidsDocument21 pagesUterine FibroidsPrasun BiswasNo ratings yet
- Abnormal Uterine Bleeding Patterns and EvaluationDocument28 pagesAbnormal Uterine Bleeding Patterns and EvaluationirmaarmiyahNo ratings yet
- MenorrhagiaDocument4 pagesMenorrhagiaFlloyd_Martin__1259No ratings yet
- Anatomy of the Urinary Bladder and UrethraDocument24 pagesAnatomy of the Urinary Bladder and Urethraمحمد حميدانNo ratings yet
- EndometriosisDocument46 pagesEndometriosisManoj Ranadive0% (1)
- Uterus NeoDocument11 pagesUterus NeoHester Marie SimpiaNo ratings yet
- ALARMER Dystocia PDFDocument5 pagesALARMER Dystocia PDFwilliamNo ratings yet
- AFE, RUPTURE OF UTERUS, (Autosaved)Document31 pagesAFE, RUPTURE OF UTERUS, (Autosaved)maezu100% (1)
- Menstrual Disorder and Abnormal BleedingDocument9 pagesMenstrual Disorder and Abnormal Bleedingdr_asalehNo ratings yet
- Tenny Parker Change A Reflection of Placental Pathology PDFDocument4 pagesTenny Parker Change A Reflection of Placental Pathology PDFEditors100% (1)
- Hysterectomy: The American College of Obstetricians and GynecologistsDocument0 pagesHysterectomy: The American College of Obstetricians and Gynecologistsmonir61No ratings yet
- Paper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionDocument14 pagesPaper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionAimanNo ratings yet
- Clinical Presentation of FibroidsDocument12 pagesClinical Presentation of FibroidsErwin YanthoNo ratings yet
- Uterine Fibroid Treatment OptionsDocument20 pagesUterine Fibroid Treatment OptionscopperNo ratings yet
- Endoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and ComplicationsDocument16 pagesEndoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and Complicationsselatur100% (1)
- Ectopic Pregnancy: by Amielia Mazwa Rafidah Obstetric and Gynecology DepartmentDocument43 pagesEctopic Pregnancy: by Amielia Mazwa Rafidah Obstetric and Gynecology DepartmentAlrick AsentistaNo ratings yet
- Monday PresentationsDocument20 pagesMonday PresentationsSunaina BhartiNo ratings yet
- MENSTRUAL DISORDERS: CAUSES, DIAGNOSIS AND MANAGEMENTDocument36 pagesMENSTRUAL DISORDERS: CAUSES, DIAGNOSIS AND MANAGEMENTAkinbani MoyosoreNo ratings yet
- Acute Kidney Injury: Causes and DiagnosisDocument37 pagesAcute Kidney Injury: Causes and DiagnosisEndah Risky GustiyantiNo ratings yet
- L The Importance of Emergency ContraceptionDocument20 pagesL The Importance of Emergency ContraceptionAsma BegumNo ratings yet
- Benign Breast DiseasesDocument24 pagesBenign Breast DiseasesNur Hanani KhanNo ratings yet
- Hysteroscopic Limitations PDFDocument59 pagesHysteroscopic Limitations PDFV R100% (1)
- Impey Obs and Gynae Revision Notes PDFDocument9 pagesImpey Obs and Gynae Revision Notes PDFRoiseNo ratings yet
- Day Care SurgeryDocument5 pagesDay Care SurgeryazharmoNo ratings yet
- Polycystic Ovarian Syndrome: Dr. PrabhavathiDocument30 pagesPolycystic Ovarian Syndrome: Dr. PrabhavathiKasi PrasadNo ratings yet
- Hormonal ContraceptivesDocument25 pagesHormonal Contraceptivesmd easarur rahmanNo ratings yet
- Overview of Benign Breast DiseaseDocument12 pagesOverview of Benign Breast DiseaseGabriela Zavaleta CamachoNo ratings yet
- Gynecological Ultrasound Basic2Document145 pagesGynecological Ultrasound Basic2Mahmoud Saeed100% (1)
- 11abnormal Uterine BleedingDocument32 pages11abnormal Uterine BleedingAkinbani MoyosoreNo ratings yet
- HysterosDocument17 pagesHysterosAnto PopaNo ratings yet
- Cervical Intraepithelial Neoplasia and Cervical CancerDocument28 pagesCervical Intraepithelial Neoplasia and Cervical CancerNatnael100% (1)
- Operative GynaecologyDocument59 pagesOperative GynaecologyArun Shree R0% (1)
- Phyllodes TumorDocument20 pagesPhyllodes TumorManuela KarinaaNo ratings yet
- 8surgical Management of Dysfunctional Uterine Bleeding - KabilanDocument14 pages8surgical Management of Dysfunctional Uterine Bleeding - KabilanNavani TharanNo ratings yet
- Pathology of The AdnexaDocument59 pagesPathology of The AdnexaArnella HutagalungNo ratings yet
- Medical and Surgical Management: of Uterine LeiomyomasDocument78 pagesMedical and Surgical Management: of Uterine LeiomyomasMarthinKolelupunNo ratings yet
- Mirizzi Syndrome: An Unusual Presentation of CholecystitisDocument16 pagesMirizzi Syndrome: An Unusual Presentation of CholecystitisAnn Alegre ValenzuelaNo ratings yet
- Sterility and Its TreaerrrtmentDocument11 pagesSterility and Its TreaerrrtmentFares EL DeenNo ratings yet
- Abnormal Uterine BleedingDocument5 pagesAbnormal Uterine Bleedingwuryan dewiNo ratings yet
- Urethral InjuryDocument56 pagesUrethral InjuryParty NoriNo ratings yet
- POstmenopausal BleedingDocument62 pagesPOstmenopausal BleedingIdham BaharudinNo ratings yet
- Evaluation of The Endometrium For Malignant or Premalignant DiseaseDocument10 pagesEvaluation of The Endometrium For Malignant or Premalignant Diseasenautilus81No ratings yet
- Management of Benign Breast Conditions: Part 2 - Breast Lumps and LesionsDocument3 pagesManagement of Benign Breast Conditions: Part 2 - Breast Lumps and Lesionspeter_mrNo ratings yet
- Ocular Manifestations in AIDSDocument27 pagesOcular Manifestations in AIDSAnumeha Jindal100% (1)
- Leiomioma - TratamientoDocument37 pagesLeiomioma - TratamientoNella SolanoNo ratings yet
- Dilation and CurettageDocument9 pagesDilation and CurettagedenekeNo ratings yet
- Classification and Diagnosis of Endometrial Hyperplasia - UpToDateDocument24 pagesClassification and Diagnosis of Endometrial Hyperplasia - UpToDatenoor hyNo ratings yet
- Benignlesionshanisah 161129150208Document71 pagesBenignlesionshanisah 161129150208Mohammad Saadullah Khan KakarNo ratings yet
- Endometriosis: Causes, Symptoms and TreatmentDocument31 pagesEndometriosis: Causes, Symptoms and TreatmentChauthiran Agamudaiyar100% (1)
- Com Med Spotters ..Document14 pagesCom Med Spotters ..Bi PinNo ratings yet
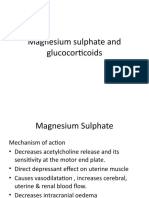
- Magnesium sulphate and glucocorticoids for preterm labor managementDocument21 pagesMagnesium sulphate and glucocorticoids for preterm labor managementBi PinNo ratings yet
- Multiple Sclerosis: Dr. Anil Dhakal MD (Internal Medicine)Document52 pagesMultiple Sclerosis: Dr. Anil Dhakal MD (Internal Medicine)Bi PinNo ratings yet
- Hyper Calc Emi ADocument26 pagesHyper Calc Emi ABi PinNo ratings yet
- Adrenal Disorders: Dr. Anil Dhakal Lecturer, Internal MedicineDocument53 pagesAdrenal Disorders: Dr. Anil Dhakal Lecturer, Internal MedicineBi PinNo ratings yet
- Copd 1Document44 pagesCopd 1Bi PinNo ratings yet
- Poisoning II FinalDocument45 pagesPoisoning II FinalBi PinNo ratings yet
- Cervical Cancer Screening and Risk FactorsDocument54 pagesCervical Cancer Screening and Risk FactorsBi PinNo ratings yet
- Orthopaedics Instruments: Kirschner WireDocument17 pagesOrthopaedics Instruments: Kirschner WireBi PinNo ratings yet
- Ortho Instruments & ImplantsDocument106 pagesOrtho Instruments & ImplantsBi PinNo ratings yet
- Cervical CancerDocument15 pagesCervical CancerMahen BoralessaNo ratings yet
- Polycystic Ovarian Syndrome: Iggy Candice Songco Resident Physician Trainee IIDocument78 pagesPolycystic Ovarian Syndrome: Iggy Candice Songco Resident Physician Trainee IIlovelots1234No ratings yet
- Schoolarship Exam MCQsDocument12 pagesSchoolarship Exam MCQsSaber AlasmarNo ratings yet
- Ebd Belum Nama AnDocument33 pagesEbd Belum Nama AnSelia PutriNo ratings yet
- Menstrual Cycle and Ovulation Period PDFDocument3 pagesMenstrual Cycle and Ovulation Period PDFSalman AmirNo ratings yet
- Pelvic Inflammatory Disease: Diagnosis, Management, and PreventionDocument8 pagesPelvic Inflammatory Disease: Diagnosis, Management, and PreventionJoão Marcelo ColunaNo ratings yet
- Department of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020Document3 pagesDepartment of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020noorNo ratings yet
- VaginitisDocument16 pagesVaginitiserfNo ratings yet
- NURSING RESEARCH-Questionnaire On Sexually Transmitted InfectionsDocument3 pagesNURSING RESEARCH-Questionnaire On Sexually Transmitted InfectionsEJ Cubero, R☤NNo ratings yet
- MenopauseDocument20 pagesMenopausepolen deoneNo ratings yet
- Breast Care and Breast Feeding For CI, by DR Abera Sept 2021Document57 pagesBreast Care and Breast Feeding For CI, by DR Abera Sept 2021Kerod AbebeNo ratings yet
- Duty of Candour: The Obstetrics and Gynaecology Perspective: CommentaryDocument4 pagesDuty of Candour: The Obstetrics and Gynaecology Perspective: CommentaryKeeranmayeeishraNo ratings yet
- Aogs 12055Document8 pagesAogs 12055Wendy ThamrinNo ratings yet
- Menstrual CycleDocument16 pagesMenstrual CycleDikpal BikramNo ratings yet
- B.Sc. Operation Theater Tecnology (5-6 Sem) Syllabus 2020 Batch OnwardsDocument16 pagesB.Sc. Operation Theater Tecnology (5-6 Sem) Syllabus 2020 Batch OnwardsBipun patelNo ratings yet
- Bartholin CystDocument21 pagesBartholin Cystwizborrlyzo006No ratings yet
- Ob Part 2Document7 pagesOb Part 2gmik02No ratings yet
- Research Family PlanningDocument35 pagesResearch Family PlanningMae Ann Esguerra LacsonNo ratings yet
- Laparoscopic Management of Giant Ovarian Cyst A Case ReportDocument3 pagesLaparoscopic Management of Giant Ovarian Cyst A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unit 5 Postpartum Health and Nursing Care: TOPIC 5.1, 5.2, 5.3Document23 pagesUnit 5 Postpartum Health and Nursing Care: TOPIC 5.1, 5.2, 5.3Krista KloseNo ratings yet
- Effective Treatment With Hormeel S Dosage RecommendationsDocument2 pagesEffective Treatment With Hormeel S Dosage Recommendationssurfer_No ratings yet
- Ectopic Pregnancy: Causes, Symptoms, Diagnosis and TreatmentDocument15 pagesEctopic Pregnancy: Causes, Symptoms, Diagnosis and TreatmentPrincess Huey GreyNo ratings yet
- Contraceptive Options For Women and Couples With HIV: Intrauterine Device (Iud or Iucd)Document23 pagesContraceptive Options For Women and Couples With HIV: Intrauterine Device (Iud or Iucd)Sitha MahendrataNo ratings yet
- Grade 10 Science Quarter 3 WEEK 4 I.: Menstrual-CycleDocument3 pagesGrade 10 Science Quarter 3 WEEK 4 I.: Menstrual-CycleAnn ClarisseNo ratings yet
- Abnormal Uterine ActionDocument64 pagesAbnormal Uterine ActionKanimozhi Kasinathan100% (1)
- FAMILY PLANNING PERSONAL NOTESDocument4 pagesFAMILY PLANNING PERSONAL NOTESOB-GYNE DEPARTMENTNo ratings yet