You might also like
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- GIT EmbryologyDocument39 pagesGIT Embryologyqnz78swpjmNo ratings yet
- Digestive System EmbryologyDocument104 pagesDigestive System EmbryologyAlistair WalkerNo ratings yet
- Development of Digestive SystemDocument35 pagesDevelopment of Digestive SystemPraney SlathiaNo ratings yet
- During Week 3 of Human DevelopmentDocument2 pagesDuring Week 3 of Human DevelopmentCleinne Florence Geeseler FermoNo ratings yet
- Embryology of the Gastrointestinal TractDocument58 pagesEmbryology of the Gastrointestinal TractOlatomide OlaniranNo ratings yet
- Development of the Gastrointestinal SystemDocument88 pagesDevelopment of the Gastrointestinal SystemBindiya MangarNo ratings yet
- Dr. Meidona - Development of Gastrointestinal System PDFDocument54 pagesDr. Meidona - Development of Gastrointestinal System PDFwkwkwkhhhhNo ratings yet
- The Gut Tube and Body CavitiesDocument31 pagesThe Gut Tube and Body CavitiesGeoffreyNo ratings yet
- Development of Gastrointestinal SystemDocument29 pagesDevelopment of Gastrointestinal SystemrifkaraihanaNo ratings yet
- DIgestive System EmbDocument85 pagesDIgestive System EmbDanish GujjarNo ratings yet
- Week 4 Embryology Development of Gastrointestinal: DR Marselina TanDocument29 pagesWeek 4 Embryology Development of Gastrointestinal: DR Marselina TanMaria Dini AdmiratiNo ratings yet
- Development of GITDocument34 pagesDevelopment of GITWahida Amalin Ab RazakNo ratings yet
- Embryology Course VIII - Digestive SystemDocument47 pagesEmbryology Course VIII - Digestive SystemRawa MuhsinNo ratings yet
- Embryo Development Ofthe GI SytermDocument11 pagesEmbryo Development Ofthe GI SytermKingNo ratings yet
- Body Cavities and Diaphragm 15Document21 pagesBody Cavities and Diaphragm 15Lugembe MasolaNo ratings yet
- Development of The Gi SystemDocument6 pagesDevelopment of The Gi SystemKingNo ratings yet
- Digestive SystemDocument106 pagesDigestive SystemAuza Moses IbrahimNo ratings yet
- DR - Eftekhar Shamkhee Abbood Senior Lecturer Obstetrician and Gynecologist M.B.Ch.B/Cabog Ibn-Sina University of Medical and Pharmaceutical SciencesDocument26 pagesDR - Eftekhar Shamkhee Abbood Senior Lecturer Obstetrician and Gynecologist M.B.Ch.B/Cabog Ibn-Sina University of Medical and Pharmaceutical Sciencesرلا رةنNo ratings yet
- Development of the Gastrointestinal TractDocument28 pagesDevelopment of the Gastrointestinal TractSaif100% (1)
- Anatomy of The Abdomen (1) : - IntroductionDocument21 pagesAnatomy of The Abdomen (1) : - IntroductionMunachande KanondoNo ratings yet
- Clinical Embriology and Anatomy of Gi Tract Part1Document43 pagesClinical Embriology and Anatomy of Gi Tract Part1Luna LitamiNo ratings yet
- Abdominal AnatomyDocument39 pagesAbdominal AnatomyRahul MandhanNo ratings yet
- Lo 4Document7 pagesLo 4api-3803109No ratings yet
- Yu - Git - Emb 2Document56 pagesYu - Git - Emb 2gtaha80No ratings yet
- GitDocument11 pagesGitM DAaud SAleemNo ratings yet
- Digestive SystemDocument6 pagesDigestive SystemDorence SimuntalaNo ratings yet
- 17 - Development of Foregut-Derivatives and AnomaliesDocument22 pages17 - Development of Foregut-Derivatives and AnomaliesDr.B.B.GosaiNo ratings yet
- 1 Abdominal VisceraDocument45 pages1 Abdominal VisceraMero HamedNo ratings yet
- Development of Alimentary System Part 1Document52 pagesDevelopment of Alimentary System Part 1Aarushi JainNo ratings yet
- Gastrointestinal AnatomyDocument70 pagesGastrointestinal AnatomyNatasya Ryani PurbaNo ratings yet
- Physiology of Lower GI TractDocument180 pagesPhysiology of Lower GI TractIcarus WingsNo ratings yet
- Clinical Embriology and Anatomy of Gi Tract Part1Document44 pagesClinical Embriology and Anatomy of Gi Tract Part1trianaamalia100% (1)
- BODY CAVITY DIAPHRAGM MESENTRYDocument16 pagesBODY CAVITY DIAPHRAGM MESENTRYshallonngabirano29No ratings yet
- ANAT 221 - PeritoneumDocument22 pagesANAT 221 - PeritoneumWisdom IkechukwuNo ratings yet
- MD Anatomy Guide to the StomachDocument58 pagesMD Anatomy Guide to the StomachSkinny tuberNo ratings yet
- Development of GIT - IDocument69 pagesDevelopment of GIT - IAarushi JainNo ratings yet
- 4Document9 pages4Marielle Anne TuazonNo ratings yet
- GIT Embryology OverviewDocument48 pagesGIT Embryology Overviewgtaha80No ratings yet
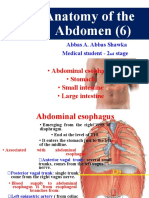
- Anatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineDocument34 pagesAnatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineBilal YimamNo ratings yet
- The StomachDocument3 pagesThe StomachAhmad BdeirNo ratings yet
- Digestive System OverviewDocument90 pagesDigestive System OverviewDiazNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFIndira Damar PangestuNo ratings yet
- Organogenetic PeriodDocument32 pagesOrganogenetic PeriodAuza Moses IbrahimNo ratings yet
- Med II GIT 2 Peritoneum Aug 23Document24 pagesMed II GIT 2 Peritoneum Aug 23Suhayb CumarNo ratings yet
- Peritoneum. Development of The Digestive System: Department of Human Anatomy Lecturer Dr. Globa LilianDocument24 pagesPeritoneum. Development of The Digestive System: Department of Human Anatomy Lecturer Dr. Globa LilianCristina GrajdeanNo ratings yet
- Digestive System - Kelompok A4Document102 pagesDigestive System - Kelompok A4Fathoni akbarNo ratings yet
- Yu - Git - Emb 1Document67 pagesYu - Git - Emb 1gtaha80No ratings yet
- G & D Lecture 9 Development of The Gi System Part 2 Spring 2018Document42 pagesG & D Lecture 9 Development of The Gi System Part 2 Spring 2018John H. SolomonNo ratings yet
- Peritoneum: General FeaturesDocument92 pagesPeritoneum: General FeaturestuhinsinghNo ratings yet
- Large Intestine - Structure and FunctionDocument13 pagesLarge Intestine - Structure and FunctiondivyasreekanthanNo ratings yet
- Small Intestine MMCDocument65 pagesSmall Intestine MMCWorku KifleNo ratings yet
- Anatomy of GIT For PCII Students..Document106 pagesAnatomy of GIT For PCII Students..AMANUEL HABTEWOLDNo ratings yet
- Bladder Anatomy EmbryologyDocument33 pagesBladder Anatomy EmbryologyFatima Zahra Rahim ArchiNo ratings yet
- DR - Anggraini - Development of Gastrointestinal SystemDocument16 pagesDR - Anggraini - Development of Gastrointestinal SystemNofilia Citra CandraNo ratings yet
- Surgical Anatomy of PeritoneumDocument63 pagesSurgical Anatomy of PeritoneumSuvarna RajNo ratings yet
- Digestive SystemDocument64 pagesDigestive SystemAyro Business CenterNo ratings yet
- Peritoneum - Dr. QuratulainDocument40 pagesPeritoneum - Dr. QuratulainWajahat FaizNo ratings yet
- The Small Intestine-1Document38 pagesThe Small Intestine-1ChiderahNo ratings yet
- DEVELOPMENT OF THE GASTROINTESTINAL TRACTDocument50 pagesDEVELOPMENT OF THE GASTROINTESTINAL TRACTYeni100% (1)
- Muscular SystemDocument18 pagesMuscular SystemAdan ImanNo ratings yet
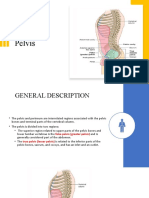
- Understanding the Pelvis and Pelvic FloorDocument35 pagesUnderstanding the Pelvis and Pelvic FloorAdan ImanNo ratings yet
- Chapter 2 GametogenesisDocument37 pagesChapter 2 GametogenesisAdan ImanNo ratings yet
- Cardiovascular System DevelopmentDocument63 pagesCardiovascular System DevelopmentAdan Iman100% (1)
- Necrotizing Enterocolitis (Sultn Aiman NeazyDocument59 pagesNecrotizing Enterocolitis (Sultn Aiman NeazyMohammed ElhashimiNo ratings yet
- GitDocument11 pagesGitM DAaud SAleemNo ratings yet
- Ninja Nerd Embryology Notes CompleteDocument111 pagesNinja Nerd Embryology Notes Completezipporahwaithera404No ratings yet
- Flashcards - GI EmbryologyDocument6 pagesFlashcards - GI EmbryologyKhanNo ratings yet
- Embryology of Digestive System1Document62 pagesEmbryology of Digestive System1Gina AnnisahNo ratings yet
- Dr. Meidona - Development of Gastrointestinal System PDFDocument54 pagesDr. Meidona - Development of Gastrointestinal System PDFwkwkwkhhhhNo ratings yet
- Digestive System: Anatomy, Functions, RegulationDocument61 pagesDigestive System: Anatomy, Functions, RegulationAanisah Ikbaar SayyidahNo ratings yet
- IB Singh Human Embryology Part 2Document547 pagesIB Singh Human Embryology Part 2Rajeshwari RajiNo ratings yet
- Sankalp Sanjeevani NEET 2024: ZoologyDocument9 pagesSankalp Sanjeevani NEET 2024: ZoologyKey RavenNo ratings yet
- Ebook Developing Human 9Th Edition Moore Test Bank Full Chapter PDFDocument30 pagesEbook Developing Human 9Th Edition Moore Test Bank Full Chapter PDFStacieSharpnocje88% (8)
- Folds of Peritoneum: Abdomen and PelvisDocument100 pagesFolds of Peritoneum: Abdomen and PelvissrisakthiNo ratings yet
- Respirator LangmanDocument10 pagesRespirator LangmanSavu MalinaNo ratings yet
- K1 - Digestive System - OverviewDocument125 pagesK1 - Digestive System - OverviewMiftachul HidayahNo ratings yet
- Endodermal Derivatives, Formation of The Gut and Its Subsequent RotationDocument14 pagesEndodermal Derivatives, Formation of The Gut and Its Subsequent RotationmikeNo ratings yet
- Structures of The ForegutDocument13 pagesStructures of The ForegutJatan KothariNo ratings yet
- Special Embryology-Norhan Ahmed Ahmed Hassan El-MeniawyDocument67 pagesSpecial Embryology-Norhan Ahmed Ahmed Hassan El-MeniawyNorhan Ahmed Ahmed Hassan El-MeniawyNo ratings yet
- Langman Medical Embryology Made EasyDocument19 pagesLangman Medical Embryology Made EasyMatet Monje96% (54)
- 3.embryonic & Fetal Period 1st Yr MedcDocument34 pages3.embryonic & Fetal Period 1st Yr MedcTofik MohammedNo ratings yet
- Embryonic Development of the Digestive SystemDocument97 pagesEmbryonic Development of the Digestive SystembarbiemeNo ratings yet
- Embryology of Respiratory System NotesDocument3 pagesEmbryology of Respiratory System NotesJulienne Sanchez-SalazarNo ratings yet
- Development of the Gastrointestinal TractDocument28 pagesDevelopment of the Gastrointestinal TractSaif100% (1)
- Esophagus & Stomach, Its Blood Supply& Development:: OesophagusDocument8 pagesEsophagus & Stomach, Its Blood Supply& Development:: OesophagusBoody KhalilNo ratings yet
- Development of Gastrointestinal SystemDocument29 pagesDevelopment of Gastrointestinal SystemrifkaraihanaNo ratings yet
- Class InsectaDocument30 pagesClass InsectaEdz SeletariaNo ratings yet
- Embryology Notes - emDocument18 pagesEmbryology Notes - emrigario80% (5)
- GIT Embryology OverviewDocument48 pagesGIT Embryology Overviewgtaha80No ratings yet
- Digestive System of Silkworm LarvaDocument17 pagesDigestive System of Silkworm LarvaRaghvendra NiranjanNo ratings yet
- DEVELOPMENT OF THE GASTROINTESTINAL TRACTDocument50 pagesDEVELOPMENT OF THE GASTROINTESTINAL TRACTYeni100% (1)
- Vipin Sharma Embryogenesis of Respiratory SystemDocument31 pagesVipin Sharma Embryogenesis of Respiratory SystemRitvik SharmaNo ratings yet
- Development of the Digestive System from Foregut to HindgutDocument90 pagesDevelopment of the Digestive System from Foregut to Hindgutyusrah mukhtarNo ratings yet