You might also like
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
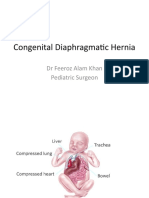
- Congenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonDocument21 pagesCongenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonPrabhat GuptaNo ratings yet
- Congenital Diaphragmatic HerniaDocument45 pagesCongenital Diaphragmatic HerniaDabessa MosissaNo ratings yet
- Nursing Care of Patients With Pneumothorax: Prepared By: N. WadeDocument33 pagesNursing Care of Patients With Pneumothorax: Prepared By: N. WadeokaciaNo ratings yet
- Respiratory EmergencyDocument187 pagesRespiratory EmergencyHemraj SoniNo ratings yet
- Chylothorax Pseudochylotho RAX: DR - Kalpesh Patel Junior Resident TBHPDocument67 pagesChylothorax Pseudochylotho RAX: DR - Kalpesh Patel Junior Resident TBHPYohelio Priawan SibuNo ratings yet
- Cyanotic Congenital Heart DiseaseDocument6 pagesCyanotic Congenital Heart DiseaseSimran JosanNo ratings yet
- Chylothorax Pseudochylotho RAXDocument67 pagesChylothorax Pseudochylotho RAXWadezigNo ratings yet
- Paediatric AnsDocument142 pagesPaediatric AnsAbdulkadir HasanNo ratings yet
- Pediatric SurgeryDocument60 pagesPediatric SurgeryAbdalla SamatarNo ratings yet
- Paediatric Chest RadiologyDocument120 pagesPaediatric Chest Radiologysunielgoel100% (6)
- Development of The Respiratory SystemDocument22 pagesDevelopment of The Respiratory SystemtuhinNo ratings yet
- Ass. of NewbornDocument54 pagesAss. of NewbornMahad Maxamed AxmedNo ratings yet
- Differential Diagnosis of Pleural Effusion-82892Document56 pagesDifferential Diagnosis of Pleural Effusion-82892Salih AslaNo ratings yet
- Nelson's Club - AtelectasisDocument22 pagesNelson's Club - AtelectasisAyen FornollesNo ratings yet
- Respiratory Distress SyndromeDocument121 pagesRespiratory Distress Syndromeinno so qtNo ratings yet
- Duodenal Obstruction: Dr. Mochamad Reza FebrianDocument24 pagesDuodenal Obstruction: Dr. Mochamad Reza FebrianBoby ChandraNo ratings yet
- Diaphragmatic HerniaDocument42 pagesDiaphragmatic Herniahayssam rashwan50% (2)
- Tetralogy of FallotDocument26 pagesTetralogy of FallotGI SanadaNo ratings yet
- Hernia DiafragmaDocument7 pagesHernia Diafragmasentaro2100% (1)
- Pedi 2Document25 pagesPedi 2Roba ANo ratings yet
- Tetraogy of FallotDocument9 pagesTetraogy of FallotMary Louise MadariagaNo ratings yet
- Congenital Anomalies of Airway and Lung ParenchymaDocument71 pagesCongenital Anomalies of Airway and Lung ParenchymaGopal ChawlaNo ratings yet
- Pediatric Surgery Dr. A. IgamaDocument6 pagesPediatric Surgery Dr. A. IgamaMarco Paulo Reyes NaoeNo ratings yet
- Prolaps Tali PusatDocument10 pagesProlaps Tali PusatYona Yohana SNo ratings yet
- HydrocephalusDocument39 pagesHydrocephalusAjeng Aristiany Rahawarin100% (1)
- Neonatal Physiology: Teka Siebenaler RRT Cardiopulmonary Services University of Minnesota Amplatz Children's HospitalDocument29 pagesNeonatal Physiology: Teka Siebenaler RRT Cardiopulmonary Services University of Minnesota Amplatz Children's HospitalStrept PneumoniaNo ratings yet
- Abdominal Wall Defects PresentationDocument45 pagesAbdominal Wall Defects PresentationWasswaNo ratings yet
- Common Congenital Git Malformations FinDocument60 pagesCommon Congenital Git Malformations FinRuth DanielNo ratings yet
- 51episiotomyDocument21 pages51episiotomyJay SeetohulNo ratings yet
- Duodenal ObstructionDocument53 pagesDuodenal ObstructionBoby ChandraNo ratings yet
- GI NotesDocument36 pagesGI Noteswmtxbb100% (1)
- Esophageal Atresia & Tracheo-Esophageal Fistula: HENG Sophea, MDDocument67 pagesEsophageal Atresia & Tracheo-Esophageal Fistula: HENG Sophea, MDchivorn.ch123No ratings yet
- Neonatal InjuriesDocument79 pagesNeonatal InjuriesEdward Munyaradzi KutsanziraNo ratings yet
- Presentation-WPS OfficeDocument30 pagesPresentation-WPS OfficeKinjal VasavaNo ratings yet
- 51 EpisiotomyDocument21 pages51 Episiotomydr_asaleh100% (2)
- Surgry Lecture For Medical Studentes: By: Shitahun ADocument37 pagesSurgry Lecture For Medical Studentes: By: Shitahun ASisay FentaNo ratings yet
- A Cyst in Lung (CPC)Document64 pagesA Cyst in Lung (CPC)Javaid Khan100% (1)
- GitDocument11 pagesGitM DAaud SAleemNo ratings yet
- Tracheoesophageal Fistula: DR - Yamuna TulasiDocument59 pagesTracheoesophageal Fistula: DR - Yamuna TulasiTulasiNo ratings yet
- HydrocephalussDocument32 pagesHydrocephalussElvisNo ratings yet
- Screenshot 2022-05-30 at 9.43.21 PMDocument23 pagesScreenshot 2022-05-30 at 9.43.21 PMAZNo ratings yet
- AirwayDocument15 pagesAirwayYonathan asnakeNo ratings yet
- Autopsy in Maternal Death.Document41 pagesAutopsy in Maternal Death.Medicine 0786No ratings yet
- Chest TraumaDocument39 pagesChest Traumayared getachewNo ratings yet
- Abnormalities of The PuerperiumDocument59 pagesAbnormalities of The PuerperiumKENEDYNo ratings yet
- Anaesthetic Management of Paediatric Emergencies Corrected 3Document51 pagesAnaesthetic Management of Paediatric Emergencies Corrected 3oriaboseNo ratings yet
- Comparison of Transverse and Vertical Skin Incision ForDocument6 pagesComparison of Transverse and Vertical Skin Incision ForHerry SasukeNo ratings yet
- Choledochal Cyst..Document50 pagesCholedochal Cyst..Ramesh ReddyNo ratings yet
- Thoracic Decortication: Sabita Chalise Bns 3 YearDocument32 pagesThoracic Decortication: Sabita Chalise Bns 3 YearRamchandra Chalise100% (1)
- Pleura Effusion Bahan Kuliah PakarDocument27 pagesPleura Effusion Bahan Kuliah PakarAfifah NaurahNo ratings yet
- Hypoplasia of The Lung: Helmilubis Ridwanm. Daulay Wismandalimunthe RinisavitridaulayDocument29 pagesHypoplasia of The Lung: Helmilubis Ridwanm. Daulay Wismandalimunthe RinisavitridaulayM Rizky Assilmy LubisNo ratings yet
- Pleuraleffusion 160424141916Document20 pagesPleuraleffusion 160424141916Jessa AdenigNo ratings yet
- HemothoraxDocument27 pagesHemothoraxShreyasi AnkushNo ratings yet
- Empyema: By-Komal JaiswalDocument29 pagesEmpyema: By-Komal JaiswalOlga GoryachevaNo ratings yet
- 1.suppurative Lung DiseasesDocument78 pages1.suppurative Lung Diseasesrobel derejeNo ratings yet
- Pleura Effusion Bahan Kuliah PakarDocument27 pagesPleura Effusion Bahan Kuliah PakarRudy LusmiandaNo ratings yet
- Birth TraumaDocument57 pagesBirth TraumaAbu HajerahNo ratings yet
- Congenital Diaphragmatic HerniaDocument3 pagesCongenital Diaphragmatic HerniaMahmoud SalmanNo ratings yet
- Varaah KavachDocument7 pagesVaraah KavachBalagei Nagarajan100% (1)
- The Association Between Eating Disorders and Stress Among Medical Student: A Cross-Sectional StudyDocument11 pagesThe Association Between Eating Disorders and Stress Among Medical Student: A Cross-Sectional StudyIJAR JOURNALNo ratings yet
- Coastal Management NotesDocument2 pagesCoastal Management Notesapi-330338837No ratings yet
- Amies A 114 - 3Document17 pagesAmies A 114 - 3Syed Umar Farooq100% (1)
- Hygiene PassportDocument133 pagesHygiene PassportAsanga MalNo ratings yet
- Tamil NaduDocument64 pagesTamil Nadushanpaga priyaNo ratings yet
- Deva Surya - 19MF02Document30 pagesDeva Surya - 19MF02SaravananNo ratings yet
- Mwangi, Thyne, Rao - 2013 - Extensive Experimental Wettability Study in Sandstone and Carbonate-Oil-Brine Systems Part 1 - Screening ToDocument7 pagesMwangi, Thyne, Rao - 2013 - Extensive Experimental Wettability Study in Sandstone and Carbonate-Oil-Brine Systems Part 1 - Screening ToMateo AponteNo ratings yet
- Manual de Taller sk350 PDFDocument31 pagesManual de Taller sk350 PDFLeo Perez100% (1)
- Guide To Greyhawk PDFDocument108 pagesGuide To Greyhawk PDFAnonymous PtMxUHm9RoNo ratings yet
- 2.4 Assembly ManualDocument139 pages2.4 Assembly Manualgustavo dlsNo ratings yet
- Sermo 13 de Tempore (2 Feb in Praes)Document1 pageSermo 13 de Tempore (2 Feb in Praes)GeorgesEdouardNo ratings yet
- HBT vs. PHEMT vs. MESFET: What's Best and Why: Dimitris PavlidisDocument4 pagesHBT vs. PHEMT vs. MESFET: What's Best and Why: Dimitris Pavlidissagacious.ali2219No ratings yet
- Gcat Threathorizons Full Jan2023Document26 pagesGcat Threathorizons Full Jan2023josbjsNo ratings yet
- Tempera 2018 AbstractsDocument45 pagesTempera 2018 AbstractsGerard Emmanuel KamdemNo ratings yet
- Schneider Modicon M580 CatalogueDocument268 pagesSchneider Modicon M580 CatalogueKhaerul Imam HermanNo ratings yet
- Total04 Digital Version PDFDocument52 pagesTotal04 Digital Version PDFbeatriz matos67% (3)
- RE2S PE LPG CNG SPC Part 1Document32 pagesRE2S PE LPG CNG SPC Part 1Inversiones RinocellNo ratings yet
- Into The Unknown 21 Doc PDFDocument9 pagesInto The Unknown 21 Doc PDFFernando AlbuquerqueNo ratings yet
- Macleod - 1974 - Lucian's Knowledge of TheophrastusDocument2 pagesMacleod - 1974 - Lucian's Knowledge of TheophrastusSIMONE BLAIRNo ratings yet
- Vol07 1 PDFDocument275 pagesVol07 1 PDFRurintana Nalendra WarnaNo ratings yet
- Tutorial 2Document2 pagesTutorial 2Adam HakimiNo ratings yet
- Movimiento Circular, Momentun Lineal y EnergíaDocument92 pagesMovimiento Circular, Momentun Lineal y EnergíaJulio César Macías ZamoraNo ratings yet
- Master Key Utbk Saintek 2022 (Paket 3) Bahasa InggrisDocument5 pagesMaster Key Utbk Saintek 2022 (Paket 3) Bahasa InggrisRina SetiawatiNo ratings yet
- Laporan Pelayanan Rawat Jalan Tingkat Pertama (RJTP)Document10 pagesLaporan Pelayanan Rawat Jalan Tingkat Pertama (RJTP)dede komalasariNo ratings yet
- Faujifood Pakistan PortfolioDocument21 pagesFaujifood Pakistan PortfolioPradeep AbeynayakeNo ratings yet
- Ac 521 007Document10 pagesAc 521 007JacquesNo ratings yet
- Offsetting Macro-Shrinkage in Ductile IronDocument13 pagesOffsetting Macro-Shrinkage in Ductile IronmetkarthikNo ratings yet
- 14 WosDocument6 pages14 WosATUL KURZEKARNo ratings yet
- 100 Years of Hydrodynamic PDFDocument28 pages100 Years of Hydrodynamic PDFnikodjoleNo ratings yet