You might also like
- Cell Wall Inhibitor PPT SlideDocument47 pagesCell Wall Inhibitor PPT Slidekhawaja sahabNo ratings yet
- Acute Complications of Diabetes MellitusDocument1 pageAcute Complications of Diabetes MellitusGerardLum100% (1)
- Dose Adjustment in Renal and Hepatic FailureDocument27 pagesDose Adjustment in Renal and Hepatic Failurevanita100% (1)
- 4-Pharmacokinetics IDocument88 pages4-Pharmacokinetics IMarc Imhotep Cray, M.D.No ratings yet
- Pharmacotherapeutics IIIDocument8 pagesPharmacotherapeutics IIILucky NihaNo ratings yet
- Hospital Pharmacy-Lecture Notes-1Document19 pagesHospital Pharmacy-Lecture Notes-1Patras BhattiNo ratings yet
- MDS3 Ch45 HospitalPharmacyMgmt Nov2011Document17 pagesMDS3 Ch45 HospitalPharmacyMgmt Nov2011Andre SamsungNo ratings yet
- Pharmaceutical Jurisprudence ManualDocument12 pagesPharmaceutical Jurisprudence ManualSlark SlarkNo ratings yet
- Institutional Pharmacy PracticeDocument17 pagesInstitutional Pharmacy PracticeRichmond AmuraoNo ratings yet
- Cell Wall InhibitorsDocument52 pagesCell Wall InhibitorsApurba Sarker Apu100% (1)
- Introduction to Clinical PharmacyDocument54 pagesIntroduction to Clinical PharmacySajid Hassan GhafoorNo ratings yet
- Procurement and WarehouseDocument28 pagesProcurement and WarehouseVarshith Gandla100% (1)
- Basic Principles of PharmacologyDocument75 pagesBasic Principles of PharmacologyJessica Febrina Wuisan100% (1)
- Basic - Concepts - in - Pharmaceutical - Care CLINICAL PHARMACYDocument17 pagesBasic - Concepts - in - Pharmaceutical - Care CLINICAL PHARMACYPrincess RonsableNo ratings yet
- AOTA Statement On Role of OT in NICUDocument9 pagesAOTA Statement On Role of OT in NICUMapi RuizNo ratings yet
- 2013 Introduction of Clinical PharmacyDocument18 pages2013 Introduction of Clinical Pharmacyyudi100% (1)
- Drug Therapy MonitoringDocument13 pagesDrug Therapy MonitoringRaju Niraula100% (1)
- 3B - Clinical PharmacyDocument35 pages3B - Clinical PharmacyekramNo ratings yet
- 1 - Pharmaceutical Care Practice - An OverviewDocument76 pages1 - Pharmaceutical Care Practice - An OverviewekramNo ratings yet
- Patient Medication Profile and CounselingDocument56 pagesPatient Medication Profile and CounselingMeimei QueNo ratings yet
- Toxicity and Toxicokinetics of Metformin in RatsDocument26 pagesToxicity and Toxicokinetics of Metformin in RatsPooja ReddyNo ratings yet
- Clinical Pharmacy PHR 405: Chapter 1: General ConsiderationsDocument24 pagesClinical Pharmacy PHR 405: Chapter 1: General ConsiderationsSamiul Alam Rajib100% (1)
- Fundamentals of Pharmacy Prescription Practice PathDocument66 pagesFundamentals of Pharmacy Prescription Practice PathLHYRA KATHLEEN LOPEZ100% (1)
- Hospital PharmacyDocument15 pagesHospital PharmacyYet Barreda BasbasNo ratings yet
- GUIDE TO SAFE MEDICINE DISPENSINGDocument7 pagesGUIDE TO SAFE MEDICINE DISPENSINGGizelle Mae Pasiol-MacayanNo ratings yet
- Non Linear PharmacokineticsDocument94 pagesNon Linear PharmacokineticsJaspreet Guraya100% (1)
- Pharmacotherapeutics 140828123349 Phpapp02Document14 pagesPharmacotherapeutics 140828123349 Phpapp02Anonymous s9i0WyKF200% (1)
- Therapeutic Drug Monitoring GuideDocument33 pagesTherapeutic Drug Monitoring GuideDr. Raghavendra Kumar GundaNo ratings yet
- Therapeutic Drug Monitoring-FinalDocument49 pagesTherapeutic Drug Monitoring-FinalSaiesh PhaldesaiNo ratings yet
- Change Your Life in 7 Days With NLP - Paul Mckenna BrochureDocument2 pagesChange Your Life in 7 Days With NLP - Paul Mckenna Brochureapi-385316675% (4)
- Optimizing Patient Care Through Clinical PharmacyDocument14 pagesOptimizing Patient Care Through Clinical Pharmacydaniya nadeem100% (1)
- Clinical PharmacokineticsDocument31 pagesClinical PharmacokineticsArdiyanti Puspitasari100% (1)
- The Role of Clinical Pharmacist in Pharmacovigilance and Drug Safety in Teritiary Care Teaching HospitalDocument11 pagesThe Role of Clinical Pharmacist in Pharmacovigilance and Drug Safety in Teritiary Care Teaching HospitalBaru Chandrasekhar RaoNo ratings yet
- B. Informatics (Slides 1-66)Document7 pagesB. Informatics (Slides 1-66)Chrissy LayugNo ratings yet
- Comunity Pharmacy Introduction ModDocument42 pagesComunity Pharmacy Introduction ModPrity girlNo ratings yet
- Application of PK in Clinical SitutionDocument42 pagesApplication of PK in Clinical Situtionsafia mehmood100% (1)
- Question and AnswerDocument4 pagesQuestion and AnswerShaf AbubakarNo ratings yet
- Medicine Price Surveys, Analyses and Comparisons: Evidence and Methodology GuidanceFrom EverandMedicine Price Surveys, Analyses and Comparisons: Evidence and Methodology GuidanceSabine VoglerNo ratings yet
- 07 Dosage RegimenDocument44 pages07 Dosage Regimenzetttttttttt100% (3)
- Communication Skills in Pharmacy Practice: Dr. Hiwak. SaaedDocument70 pagesCommunication Skills in Pharmacy Practice: Dr. Hiwak. SaaedAnonymous whcvnPBeQNo ratings yet
- Annexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistDocument5 pagesAnnexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistGaurav Singh67% (3)
- Introduction To PharmacotherapeuticsDocument14 pagesIntroduction To Pharmacotherapeuticskyra alondayNo ratings yet
- Role of Regulatory Authorities in Clinical TrialsDocument8 pagesRole of Regulatory Authorities in Clinical TrialsAnish GhaleNo ratings yet
- Pharmacology in Drug Discovery: Understanding Drug ResponseFrom EverandPharmacology in Drug Discovery: Understanding Drug ResponseNo ratings yet
- SSIPDocument4 pagesSSIPGlenn Clemente100% (2)
- Hospital Pharmacy RolesDocument11 pagesHospital Pharmacy RoleskingkooooongNo ratings yet
- Ward Round Participation Benefits for PharmacistsDocument2 pagesWard Round Participation Benefits for PharmacistsAnonymous whcvnPBeQNo ratings yet
- BIOAVAILABILITY AND BIOEQUIVALANCE STUDIES Final - PPTX'Document32 pagesBIOAVAILABILITY AND BIOEQUIVALANCE STUDIES Final - PPTX'Md TayfuzzamanNo ratings yet
- Code of Ethics for Kenyan PharmacistsDocument20 pagesCode of Ethics for Kenyan PharmacistsKevin Chapley50% (2)
- Prodrug Delivery: A Concise OverviewDocument6 pagesProdrug Delivery: A Concise OverviewanantachoudhuryNo ratings yet
- Pharmacotherapy of HTNDocument57 pagesPharmacotherapy of HTNAbera JamboNo ratings yet
- Bronchodilator & Other Drugs Used in AsthmaDocument15 pagesBronchodilator & Other Drugs Used in AsthmaGenta JagadNo ratings yet
- HOSPITAL AND CLINICAL PHARMCAY QuestionsDocument20 pagesHOSPITAL AND CLINICAL PHARMCAY Questionslola&losa farhanNo ratings yet
- 3B - Clinical PharmacyDocument35 pages3B - Clinical PharmacyekramNo ratings yet
- Clinical PharmacyDocument15 pagesClinical PharmacyKate EvangelistaNo ratings yet
- General Pharmacology - Sources of Drugs and Routes of AdministrationDocument48 pagesGeneral Pharmacology - Sources of Drugs and Routes of AdministrationDhriti Brahma78% (9)
- Immunization Policy Guidline - Kenya 2013Document72 pagesImmunization Policy Guidline - Kenya 2013okwadha simionNo ratings yet
- Pharmacists Role Clinical Pharmacokinetic MonitoringDocument2 pagesPharmacists Role Clinical Pharmacokinetic MonitoringauliaNo ratings yet
- Introduction To Pharmacy PracticeDocument9 pagesIntroduction To Pharmacy PracticeRai Waqas100% (1)
- Model Pharmacy GuidelinesDocument36 pagesModel Pharmacy GuidelinesSabbir Ismail50% (2)
- Biopharmaceutics and PharmacokineticDocument4 pagesBiopharmaceutics and PharmacokineticRiyaz AliNo ratings yet
- Introduction To PharmacologyDocument28 pagesIntroduction To Pharmacologynadar shahNo ratings yet
- Autacoid PharmacologyDocument38 pagesAutacoid PharmacologyAakkkNo ratings yet
- Pharmacology Practical Manual - Student Copy2Document11 pagesPharmacology Practical Manual - Student Copy2NareshNo ratings yet
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- Quality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDocument37 pagesQuality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDewi ListyoriniNo ratings yet
- BPN Datangi MalaysiaDocument62 pagesBPN Datangi MalaysiaafandianddonkeyNo ratings yet
- Evaluation and Treatment of Aphasia Among The Elderly With StrokeDocument11 pagesEvaluation and Treatment of Aphasia Among The Elderly With StrokemgpastorNo ratings yet
- Caldorol (Ibuprofen IV)Document14 pagesCaldorol (Ibuprofen IV)Agus SusantoNo ratings yet
- UG MaharashtraNationalLawUniversityMNLUMumbaiDocument5 pagesUG MaharashtraNationalLawUniversityMNLUMumbaiArpan KushwahaNo ratings yet
- A Study To Assess The Effectiveness of Hydrabadi Mix Ball On Nutritional Status Among Malnourished Under Five Year Children at Selected Anganwadi in Barabanki, Uttar PradeshDocument15 pagesA Study To Assess The Effectiveness of Hydrabadi Mix Ball On Nutritional Status Among Malnourished Under Five Year Children at Selected Anganwadi in Barabanki, Uttar PradeshEditor IJTSRDNo ratings yet
- BCS Class of DrugsDocument45 pagesBCS Class of DrugsLionO50% (2)
- POne MPFFL 7 RV VPSX LQRPDocument3 pagesPOne MPFFL 7 RV VPSX LQRPRavi KumarNo ratings yet
- Travel Guide to Thailand in 2021Document14 pagesTravel Guide to Thailand in 2021Russell KhanNo ratings yet
- Display PDFDocument8 pagesDisplay PDFSri BalajiNo ratings yet
- Exercises For Task 3 InglesDocument3 pagesExercises For Task 3 InglesNoelia De Los SantosNo ratings yet
- Chapter 1 2 3Document77 pagesChapter 1 2 3Ferissa MohammadNo ratings yet
- Efectos AdversosDocument10 pagesEfectos Adversosjeimmy dulceyNo ratings yet
- Guided Reflection 2Document4 pagesGuided Reflection 2Summer SeedsNo ratings yet
- EGZOTech Luna EMG Brochure 2018 With LogoDocument13 pagesEGZOTech Luna EMG Brochure 2018 With LogoApostolis KopoukisNo ratings yet
- Connectors 2Document14 pagesConnectors 2Irene SánchezNo ratings yet
- Product SelectionDocument5 pagesProduct Selectionemmanuelgk100No ratings yet
- Power of The Pinch Pinch Lower Lid BlepharoplastyDocument6 pagesPower of The Pinch Pinch Lower Lid BlepharoplastyBFF BotoxNo ratings yet
- Nursing Care Plans for Respiratory and Circulatory IssuesDocument5 pagesNursing Care Plans for Respiratory and Circulatory IssuesApryll Kristin Villaluna ZafeNo ratings yet
- Daily Ward AssignmentsDocument4 pagesDaily Ward AssignmentsMia Labrador Sta CruzNo ratings yet
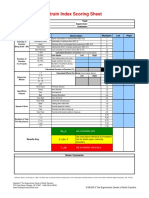
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Round Hill Community Garden FAQ - Round Hill, VirginiaDocument3 pagesRound Hill Community Garden FAQ - Round Hill, VirginiaZafiriou MavrogianniNo ratings yet
- (Bio 024) Lab Activity 12 - BloodDocument9 pages(Bio 024) Lab Activity 12 - Bloodelaq dr100% (1)
- Dr.maimoona - Gynecology-محولDocument6 pagesDr.maimoona - Gynecology-محولAbdelNasser TawfiekNo ratings yet