You might also like
- Search For TruthDocument64 pagesSearch For TruthJay Cal100% (5)
- CLDH-EI BSN 4A Fundamentals Nursing GuideDocument4 pagesCLDH-EI BSN 4A Fundamentals Nursing GuideCamille Honeyleith Lanuza FernandoNo ratings yet
- Completed Concept MapDocument4 pagesCompleted Concept Mapapi-607361848No ratings yet
- New Born Care 1Document12 pagesNew Born Care 1Tsuyoshi BangNo ratings yet
- Acid Base Balance: Carol Johns, MSN, RNDocument36 pagesAcid Base Balance: Carol Johns, MSN, RNkatrinasdNo ratings yet
- Stone Fox BookletDocument19 pagesStone Fox Bookletapi-220567377100% (3)
- Nursing ProcessDocument12 pagesNursing Processgrey26No ratings yet
- PEDS Final Questions ATI Questions and AnswersDocument14 pagesPEDS Final Questions ATI Questions and Answersianshirow834No ratings yet
- Nursing MetaparadigmDocument5 pagesNursing MetaparadigmNikzNo ratings yet
- Final Bullets in Ncm100 97-03Document4 pagesFinal Bullets in Ncm100 97-03Brainan AquinoNo ratings yet
- What is an NCPDocument38 pagesWhat is an NCPSARAH DIANA ROSE S. MANALILI100% (1)
- Chapter 09: Photo Atlas of Drug Administration Test Bank: Multiple ChoiceDocument8 pagesChapter 09: Photo Atlas of Drug Administration Test Bank: Multiple ChoicePrettygirl716No ratings yet
- Fundamental's FinalDocument21 pagesFundamental's FinalShaunn Diesto Caberto100% (1)
- Basic Nursing Fundamentals EliminationDocument35 pagesBasic Nursing Fundamentals Eliminationlisa100% (1)
- Lucid Dreaming Fast TrackDocument3 pagesLucid Dreaming Fast TrackWulan Funblogger50% (2)
- Asepsis and Infection ControlDocument6 pagesAsepsis and Infection ControlgilissaNo ratings yet
- Cranial Nerves Study GuideDocument6 pagesCranial Nerves Study Guidevienny kayeNo ratings yet
- RN Lesson 2 Safety & Infection Control PracticeDocument39 pagesRN Lesson 2 Safety & Infection Control PracticeRuthmarie CatarajaNo ratings yet
- Assessing the integumentary system: structures, functions and relationshipsDocument199 pagesAssessing the integumentary system: structures, functions and relationshipsHyacinth Jane Dela PeñaNo ratings yet
- Quiz Bowl QuestionsDocument8 pagesQuiz Bowl QuestionsKeenan Dave RivoNo ratings yet
- FNP Final TestDocument10 pagesFNP Final TestNelson MandelaNo ratings yet
- Med Surg 2 - 10 Nursing Care of Clients With Biliary DisordersDocument4 pagesMed Surg 2 - 10 Nursing Care of Clients With Biliary DisordersMaxinne RoseñoNo ratings yet
- Maternal NursingDocument16 pagesMaternal NursingJayCesarNo ratings yet
- Testing Strategies For The Nclex-Rn Examination: Chapter OneDocument22 pagesTesting Strategies For The Nclex-Rn Examination: Chapter OneShiraishiNo ratings yet
- Nursing Process Diagnosis Plan Implementation EvaluationDocument59 pagesNursing Process Diagnosis Plan Implementation EvaluationYemaya84No ratings yet
- ActiveLearningTemplate SysdisDocument1 pageActiveLearningTemplate SysdisCovey delacruzNo ratings yet
- ST ND RDDocument12 pagesST ND RDwaterbuglilyNo ratings yet
- Draft: Jurisprudence Learning Module & ExaminationDocument45 pagesDraft: Jurisprudence Learning Module & ExaminationDeepanshi RajputNo ratings yet
- Clinical Judgement-An Essential Tool in The Nursing Profession PDFDocument10 pagesClinical Judgement-An Essential Tool in The Nursing Profession PDFNers SenNo ratings yet
- Clinical Nursing JudgmentDocument7 pagesClinical Nursing Judgmentapi-502994344No ratings yet
- Health Ass ReviewerDocument8 pagesHealth Ass ReviewerchristinejeancenabreNo ratings yet
- Nursingprocess Assessing 111105015609 Phpapp01Document71 pagesNursingprocess Assessing 111105015609 Phpapp01ALmik HussinNo ratings yet
- Health AssessmentDocument51 pagesHealth AssessmentJared Dela cruzNo ratings yet
- Medical Surgical ATI Proctored Exam 2019 Questions and Answers Verified 100Document7 pagesMedical Surgical ATI Proctored Exam 2019 Questions and Answers Verified 100ianshirow834No ratings yet
- Thorax, Skin, Hair, Nails ObjectivesDocument3 pagesThorax, Skin, Hair, Nails Objectivesctramel001100% (1)
- Preparation Worksheets For NUR 345 Heart Failure SimDocument14 pagesPreparation Worksheets For NUR 345 Heart Failure SimclarimerNo ratings yet
- Concept Map TemplateDocument16 pagesConcept Map Templatenursing concept mapsNo ratings yet
- Chapter 20: Postpartum Physiologic Changes Lowdermilk: Maternity & Womens Health Care, 11th EditionDocument11 pagesChapter 20: Postpartum Physiologic Changes Lowdermilk: Maternity & Womens Health Care, 11th EditionNurse UtopiaNo ratings yet
- BulletsDocument41 pagesBulletsrosepearl ignacioNo ratings yet
- Concept MapDocument13 pagesConcept MapIssa RomaNo ratings yet
- Antepartum 1Document3 pagesAntepartum 1Emily DavisNo ratings yet
- ChartingDocument1 pageChartingAdrianaMarreroNo ratings yet
- Chapter 25: Assessment: Respiratory System Harding: Lewis's Medical-Surgical Nursing, 11th EditionDocument9 pagesChapter 25: Assessment: Respiratory System Harding: Lewis's Medical-Surgical Nursing, 11th EditionKrishna RamaNo ratings yet
- Diagnosis Schizophrenia 2Document1 pageDiagnosis Schizophrenia 2Bukola OgunnaikeNo ratings yet
- Introduction To PathophysiologyDocument125 pagesIntroduction To PathophysiologyJes CmtNo ratings yet
- Scr110-Required Reading Sp21 Fa-1Document7 pagesScr110-Required Reading Sp21 Fa-1Nur NaherNo ratings yet
- 11 Test Taking Tips & Strategies For Nurses 101Document5 pages11 Test Taking Tips & Strategies For Nurses 101xaileenxNo ratings yet
- Power Git EndoDocument170 pagesPower Git Endoapi-3735995100% (1)
- Chapter 46: Nursing Management: Renal and Urologic Problems Test BankDocument13 pagesChapter 46: Nursing Management: Renal and Urologic Problems Test BankPrince K. TaileyNo ratings yet
- Health AssessmentsDocument76 pagesHealth AssessmentsAtashia Rain GaguiNo ratings yet
- Flash Cards Vocab For Exam 1. Jarvis CH 1-3, 8, 9, 12, 13http - P.quizlet - Com - Settitle Health Assessment Vocab For Exam 1Document22 pagesFlash Cards Vocab For Exam 1. Jarvis CH 1-3, 8, 9, 12, 13http - P.quizlet - Com - Settitle Health Assessment Vocab For Exam 1tipredd100% (1)
- Alteration in OxygenationDocument8 pagesAlteration in Oxygenationraquel maniegoNo ratings yet
- Patient Rights & Organizational EthicsDocument17 pagesPatient Rights & Organizational EthicsBOnn EljayNo ratings yet
- HESI LPN ADN ENTRANCE EXAM MOBILITY EXAMS A GRADED 100 VERIFIED - pdf-1-33Document33 pagesHESI LPN ADN ENTRANCE EXAM MOBILITY EXAMS A GRADED 100 VERIFIED - pdf-1-33erick kanyiNo ratings yet
- Cardiovascular System: Claire R. Hatton, RN, MANDocument63 pagesCardiovascular System: Claire R. Hatton, RN, MANrhimineecat71No ratings yet
- English ReviewDocument8 pagesEnglish ReviewC SmithNo ratings yet
- Medical Abbreviations Cheat Sheet for NursesDocument2 pagesMedical Abbreviations Cheat Sheet for NursescarlyNo ratings yet
- Fundamentals of Nursing (Part 1)Document11 pagesFundamentals of Nursing (Part 1)Louie ParillaNo ratings yet
- Health Assessment: Nursing ProcessDocument7 pagesHealth Assessment: Nursing ProcessAngelrica TumbadoNo ratings yet
- Exam 1 Study Guide Module Nursing Art ScienceDocument33 pagesExam 1 Study Guide Module Nursing Art Scienceitschloeb100% (1)
- NCLEX 15 WK 1critical ThinkingDocument2 pagesNCLEX 15 WK 1critical ThinkingNikita TamrakarNo ratings yet
- Fundamentals of Nursing 1Document8 pagesFundamentals of Nursing 1Yrrej AtiliuqlaNo ratings yet
- Presented By: Anjani.S.Kamal 1 Year MSC (N)Document23 pagesPresented By: Anjani.S.Kamal 1 Year MSC (N)shubham vermaNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Registered Professional Nurse: Passbooks Study GuideFrom EverandRegistered Professional Nurse: Passbooks Study GuideNo ratings yet
- Assessing Head, Face and NeckDocument112 pagesAssessing Head, Face and NeckHyacinth Jane Dela PeñaNo ratings yet
- Assessing Eyes and EarsDocument156 pagesAssessing Eyes and EarsHyacinth Jane Dela PeñaNo ratings yet
- Assessing The BreastDocument37 pagesAssessing The BreastHyacinth Jane Dela PeñaNo ratings yet
- Assessment of the Female and Male Genitourinary SystemsDocument110 pagesAssessment of the Female and Male Genitourinary SystemsHyacinth Jane Dela Peña100% (1)
- I. BASIC ASSESSMENT AND BASIC CARE PROCEDURESDocument47 pagesI. BASIC ASSESSMENT AND BASIC CARE PROCEDURESHyacinth Jane Dela PeñaNo ratings yet
- Assessing The AbdomenDocument82 pagesAssessing The AbdomenHyacinth Jane Dela PeñaNo ratings yet
- The Nursing ProcessDocument152 pagesThe Nursing ProcessHyacinth Jane Dela PeñaNo ratings yet
- Neurologic AssessmentDocument58 pagesNeurologic AssessmentHanz Alecz Q. DasmariñasNo ratings yet
- Lcasean PaperDocument6 pagesLcasean Paperkean ebeoNo ratings yet
- En Subject C08Document13 pagesEn Subject C08jmolfigueiraNo ratings yet
- DR Horton Homeowners ManualDocument80 pagesDR Horton Homeowners ManualLynn RaisesNo ratings yet
- Art of Public Speaking 11th Edition Lucas Test BankDocument25 pagesArt of Public Speaking 11th Edition Lucas Test BankBryanMillernicy100% (49)
- Greetings To EveryoneDocument2 pagesGreetings To EveryoneLouella MedinaNo ratings yet
- IT Industry in India: Indian Education SystemDocument9 pagesIT Industry in India: Indian Education SystemPradeep BommitiNo ratings yet
- Course Registration Slip MBA 2023Document3 pagesCourse Registration Slip MBA 2023Piyush RaghuwanshiNo ratings yet
- ProComp 2 Service Manual SM7008P-01Document22 pagesProComp 2 Service Manual SM7008P-01cobramcNo ratings yet
- Route StructureDocument3 pagesRoute StructureAndrei Gideon ReyesNo ratings yet
- The Routledge Handbook of Translation and Culture by Sue-Ann Harding (Editor), Ovidi Carbonell Cortés (Editor)Document656 pagesThe Routledge Handbook of Translation and Culture by Sue-Ann Harding (Editor), Ovidi Carbonell Cortés (Editor)Rita PereiraNo ratings yet
- Quam SingulariDocument2 pagesQuam SingulariMichael WurtzNo ratings yet
- PNB's Financial Inclusion Initiatives and TechnologiesDocument18 pagesPNB's Financial Inclusion Initiatives and TechnologiesShreya DubeyNo ratings yet
- Asian Studies Vol 49 No 2 - 2013Document218 pagesAsian Studies Vol 49 No 2 - 2013Ari Dodol100% (1)
- Jack Turner - Not On Any MapDocument13 pagesJack Turner - Not On Any MapormrNo ratings yet
- (1902) The Centennial of The United States Military Academy at West Point New YorkDocument454 pages(1902) The Centennial of The United States Military Academy at West Point New YorkHerbert Hillary Booker 2nd100% (1)
- SGT Vacancy ListDocument196 pagesSGT Vacancy ListSusheelabaiNo ratings yet
- Estimation and Costing - LigDocument30 pagesEstimation and Costing - LigR SumithraNo ratings yet
- Mathematics Engagement in An Australian Lower Secondary SchoolDocument23 pagesMathematics Engagement in An Australian Lower Secondary SchoolDane SinclairNo ratings yet
- A Study On Customer Satisfaction of TVS Apache RTR 160Document11 pagesA Study On Customer Satisfaction of TVS Apache RTR 160Manajit BhowmikNo ratings yet
- Body PlanesDocument32 pagesBody PlanesStefanny Paramita EupenaNo ratings yet
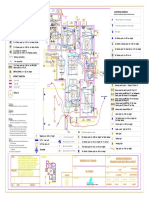
- Varun Valanjeri Electrical Layout-3Document1 pageVarun Valanjeri Electrical Layout-3ANOOP R NAIRNo ratings yet
- Keerai BenefitsDocument3 pagesKeerai BenefitsjnaguNo ratings yet
- Progress Test 1B (Units 1-3)Document6 pagesProgress Test 1B (Units 1-3)SvetlanaNo ratings yet
- RFC Mantis II Reader Data Sheet (2005)Document2 pagesRFC Mantis II Reader Data Sheet (2005)Tim BresienNo ratings yet
- Shahrzadgh InquiryassignmentDocument5 pagesShahrzadgh Inquiryassignmentapi-274076411No ratings yet