You might also like
- 8.8.2017 - Fracture of FemurDocument57 pages8.8.2017 - Fracture of FemurUlfa Sari Al-BahmiNo ratings yet
- Hip Disorders in Children: Postgraduate Orthopaedics SeriesFrom EverandHip Disorders in Children: Postgraduate Orthopaedics SeriesRating: 3 out of 5 stars3/5 (2)
- Deep Vein Thrombosis: Case PresentationDocument19 pagesDeep Vein Thrombosis: Case PresentationFebriadi RNo ratings yet
- Posterior Tibial Tendon Dysfunction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPosterior Tibial Tendon Dysfunction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Hip PathologiesDocument35 pagesHip PathologiesJoe KhdeirNo ratings yet
- Perthes DiseaseDocument45 pagesPerthes DiseaseAh ZhangNo ratings yet
- Hand Conditions and Examinations: a Rheumatologic and Orthopaedic ApproachFrom EverandHand Conditions and Examinations: a Rheumatologic and Orthopaedic ApproachNo ratings yet
- Diagnostico y Tratamiento de Tendinitis y TendinosisDocument7 pagesDiagnostico y Tratamiento de Tendinitis y TendinosisMatias ListaNo ratings yet
- 12 9 10 - PeltzDocument66 pages12 9 10 - Peltzagha_sajjad90No ratings yet
- Andi Rahmat Hidayat C 111 07 104 Advisor: Dr. Andi Sirfa Dr. Helmiyadi Kuswardhana Supervisor: Dr. Henry Yurianto, M.Phill, PHD, SP - OtDocument30 pagesAndi Rahmat Hidayat C 111 07 104 Advisor: Dr. Andi Sirfa Dr. Helmiyadi Kuswardhana Supervisor: Dr. Henry Yurianto, M.Phill, PHD, SP - OtAndi Rahmat HidayatNo ratings yet
- Supracondylar FractureDocument10 pagesSupracondylar FractureHemanath SinnathambyNo ratings yet
- ContohDocument12 pagesContohNazliah SyarbinNo ratings yet
- Rheumatoid Arthritis and AnaesthesiaDocument7 pagesRheumatoid Arthritis and AnaesthesiaAbante_gammaNo ratings yet
- Artritis Reumatoride y AnestesiaDocument7 pagesArtritis Reumatoride y Anestesiamacielhinostroza9006No ratings yet
- Deep Vein Thrombosis & Its ProphylaxisDocument90 pagesDeep Vein Thrombosis & Its ProphylaxisPratik KumarNo ratings yet
- Pulmonary EmbolismDocument28 pagesPulmonary EmbolismMohamedEzzNo ratings yet
- Physeal Injuries and Pediatrics Trauma: Dr. Aamar MunirDocument67 pagesPhyseal Injuries and Pediatrics Trauma: Dr. Aamar MunirSeimal MahmoodNo ratings yet
- Article 2Document9 pagesArticle 2105070201111009No ratings yet
- Congenital Dislocation of The Knee - RP's Ortho NotesDocument3 pagesCongenital Dislocation of The Knee - RP's Ortho NotesSabari NathNo ratings yet
- Ankle FracturesDocument47 pagesAnkle FracturesAbhishek UpadhyayNo ratings yet
- Avascular Necrosis of Femoral HeadDocument50 pagesAvascular Necrosis of Femoral HeadStar CruiseNo ratings yet
- Proximal Femoral Epiphyseal Diseases - OrthopedicsDocument12 pagesProximal Femoral Epiphyseal Diseases - OrthopedicsMuhammad ArshadNo ratings yet
- Pott DiseaseDocument15 pagesPott DiseasejunkirinNo ratings yet
- Paediatric OrthopaedicDocument77 pagesPaediatric Orthopaedicdr_asalehNo ratings yet
- Patofisiologi Ulkus VarikosumDocument5 pagesPatofisiologi Ulkus VarikosumLidya ChristyNo ratings yet
- Appendicitis: Dr. Aplin I, SPBDocument12 pagesAppendicitis: Dr. Aplin I, SPBAyu Kusuma NingrumNo ratings yet
- Deep Vein ThrombosisDocument13 pagesDeep Vein Thrombosisusmle prepNo ratings yet
- Deep Venous Thrombosis Harrison'sDocument3 pagesDeep Venous Thrombosis Harrison'sMaria Agustina Sulistyo WulandariNo ratings yet
- Case Report (Ola)Document44 pagesCase Report (Ola)amel015No ratings yet
- FRACTURES AND ITS MANAGEMENT - by Prof M Ayoub Laghari 24-4-2013Document40 pagesFRACTURES AND ITS MANAGEMENT - by Prof M Ayoub Laghari 24-4-2013SeyfNo ratings yet
- Grade 2 InfectionDocument29 pagesGrade 2 InfectionshaifNo ratings yet
- Case Study - Intertrochanteric Hip FractureDocument13 pagesCase Study - Intertrochanteric Hip FractureLei Ortega100% (6)
- Deep Venous ThrombosisDocument56 pagesDeep Venous ThrombosisSrikant Konchada100% (1)
- Amputation: DefinitionDocument9 pagesAmputation: DefinitionCharaNo ratings yet
- DR - O. K. A. SamuelsDocument76 pagesDR - O. K. A. Samuelsgdudex118811No ratings yet
- ARTHRITIS TB KNEE HIP BPTDocument84 pagesARTHRITIS TB KNEE HIP BPTMiso100% (1)
- Vermiform AppendixDocument4 pagesVermiform AppendixHarun NasutionNo ratings yet
- Femur Fractures: Subtrochanteric To SupracondylarDocument35 pagesFemur Fractures: Subtrochanteric To SupracondylarAnonymous YerdOHg3szNo ratings yet
- Tuberculosis of The HipDocument33 pagesTuberculosis of The Hipmuhammad bayu wicaksonoNo ratings yet
- Anesthetic Considerations in Patients Posted For Surgery With Ankylosing SpondylitisDocument43 pagesAnesthetic Considerations in Patients Posted For Surgery With Ankylosing Spondylitisanuk_1129No ratings yet
- The Venous Ulcer Continues ToDocument8 pagesThe Venous Ulcer Continues ToAsmat BurhanNo ratings yet
- 51episiotomyDocument21 pages51episiotomyJay SeetohulNo ratings yet
- Diabetic Foot (Leg Ulcer) : Ismail Bastomi Orthopaedic and Trumatologi Moh. Hoesin Hospital Universitas SriwijayaDocument37 pagesDiabetic Foot (Leg Ulcer) : Ismail Bastomi Orthopaedic and Trumatologi Moh. Hoesin Hospital Universitas Sriwijayahello from the other sideNo ratings yet
- Epiphrenic Diverticula - Systematic ReviewDocument7 pagesEpiphrenic Diverticula - Systematic ReviewJose JavierNo ratings yet
- Fracture of Neck of FemurDocument13 pagesFracture of Neck of FemurRosemarie AbelaNo ratings yet
- Journal AslinyaDocument11 pagesJournal AslinyainNo ratings yet
- DD Case Report Elbow DislocationDocument33 pagesDD Case Report Elbow DislocationKurniawan Nur IhsanNo ratings yet
- Background: Pediatric AppendicitisDocument15 pagesBackground: Pediatric AppendicitisnikkitaihsanNo ratings yet
- Clavicle Fracture, SC Joint and Ac Joint Injury: Team IiiDocument19 pagesClavicle Fracture, SC Joint and Ac Joint Injury: Team IiiJunarto Putra TandiarrangNo ratings yet
- Anaesthetic Management of Joint Replacement SurgeriesDocument55 pagesAnaesthetic Management of Joint Replacement SurgeriesRaguNo ratings yet
- Ortho EssentialsDocument8 pagesOrtho EssentialsShoban RajNo ratings yet
- 01-Wrist and Hand InjuriesDocument18 pages01-Wrist and Hand InjuriesHiRa HaFeezNo ratings yet
- Achilles Tendon RuptureDocument28 pagesAchilles Tendon RuptureHunar QadrNo ratings yet
- Lecture 7 Upper Limb FracturesDocument43 pagesLecture 7 Upper Limb Fracturesmukhtar abddiNo ratings yet
- Nutritional Support in Adults With Chyle LeaksDocument23 pagesNutritional Support in Adults With Chyle LeaksGleice ReinertNo ratings yet
- Pathological FractureDocument92 pagesPathological FractureSeptyAuliaNo ratings yet
- Did You Know?Document12 pagesDid You Know?ShilpaNo ratings yet
- ProspectusDocument14 pagesProspectusJawad KhanNo ratings yet
- MessageDocument5 pagesMessageJawad KhanNo ratings yet
- Management of Aseptic Tibial NonunionDocument11 pagesManagement of Aseptic Tibial NonunionJawad KhanNo ratings yet
- OsteosarcomaDocument11 pagesOsteosarcomaJawad KhanNo ratings yet
- Cemented Total Hip Arthroplasty With Autogenous Acetabular Bone Grafting For Hips With Developmental Dysplasia in AdultsDocument3 pagesCemented Total Hip Arthroplasty With Autogenous Acetabular Bone Grafting For Hips With Developmental Dysplasia in AdultsJawad KhanNo ratings yet
- PASTEST RECALL MAY May 2022Document7 pagesPASTEST RECALL MAY May 2022Jawad KhanNo ratings yet
- DR Che Writing Correction SamplesDocument67 pagesDR Che Writing Correction SamplesJawad KhanNo ratings yet
- Jan 2018+ AnsDocument28 pagesJan 2018+ AnsJawad Khan100% (2)
- Nursing Department: 551 MF Jhocson Street, Sampaloc Manila Trunkline: 712-1900 Telefax: 749-8154Document3 pagesNursing Department: 551 MF Jhocson Street, Sampaloc Manila Trunkline: 712-1900 Telefax: 749-8154Izelle FigueroaNo ratings yet
- Goldman Cardiac Risk Index CalculatorDocument4 pagesGoldman Cardiac Risk Index CalculatorCathyNo ratings yet
- Ophthalmic Viscosurgical Devices: DR A Debata DrsrpatiDocument48 pagesOphthalmic Viscosurgical Devices: DR A Debata Drsrpatidrsrp84No ratings yet
- Evd Evd Evd Evd Accudrain Accudrain Accudrain Accudrain: External Ventricular DeviceDocument1 pageEvd Evd Evd Evd Accudrain Accudrain Accudrain Accudrain: External Ventricular DeviceQueenNo ratings yet
- Arch ExpansionDocument36 pagesArch ExpansionOsama GamilNo ratings yet
- Pontics in Fixed Partial DentureDocument63 pagesPontics in Fixed Partial DentureKashish ManghaniNo ratings yet
- WWW Aegisdentalnetwork Com Id 2020 01 Primary Molar PulpotomyDocument3 pagesWWW Aegisdentalnetwork Com Id 2020 01 Primary Molar PulpotomyAlan PermanaNo ratings yet
- TraumaDocument10 pagesTraumaNur Liyana Ahmad ZakiNo ratings yet
- Lower Limb Spotters: Hip & Gluteal Region, ThighDocument6 pagesLower Limb Spotters: Hip & Gluteal Region, ThighDhaarshieth K R100% (1)
- DOC465 Laparoscopic Catalog REV NDocument152 pagesDOC465 Laparoscopic Catalog REV NlarasraeNo ratings yet
- Blepharochalasis: Clinical and Epidemiological Characteristics, Surgical Strategy and Prognosis - A Retrospective Cohort Study With 93 CasesDocument7 pagesBlepharochalasis: Clinical and Epidemiological Characteristics, Surgical Strategy and Prognosis - A Retrospective Cohort Study With 93 CasesSaqar SharepourNo ratings yet
- Intra-Muscular Route of Drug AdministrationDocument17 pagesIntra-Muscular Route of Drug AdministrationFaizah KhalidNo ratings yet
- Nursing Care of A Family When A Child Has A Cardiovascular DisorderDocument9 pagesNursing Care of A Family When A Child Has A Cardiovascular DisorderMarianne Gail100% (1)
- Mobile C Arm PortfolioDocument6 pagesMobile C Arm PortfolioAri ReviantoNo ratings yet
- Summary of Clinical RotationDocument2 pagesSummary of Clinical RotationbulikakoNo ratings yet
- ANSI Approved Standards - American National Standards (PDFDrive)Document640 pagesANSI Approved Standards - American National Standards (PDFDrive)samytamer748No ratings yet
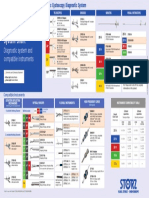
- Karl Storz Cystoscope System Chart: Diagnostic System and Compatible InstrumentsDocument1 pageKarl Storz Cystoscope System Chart: Diagnostic System and Compatible InstrumentsRaydoon SadeqNo ratings yet
- Healthy Smiles Implant Patient Surgery Information and Consent FormDocument3 pagesHealthy Smiles Implant Patient Surgery Information and Consent FormAnup Lal RajbahakNo ratings yet
- Diagnosis and Managment of Gaynecologic CancersDocument1,067 pagesDiagnosis and Managment of Gaynecologic CancersarisNo ratings yet
- JACKLER Brackmann NeurotologyDocument1,404 pagesJACKLER Brackmann NeurotologyRodrigo CabreraNo ratings yet
- Structural and Dynamic Bases of Hand Surgery by Eduardo Zancolli 1969Document1 pageStructural and Dynamic Bases of Hand Surgery by Eduardo Zancolli 1969khox0% (1)
- Assessment of Fetal Well-BeingDocument63 pagesAssessment of Fetal Well-BeingArhum Siddiqi100% (1)
- Stab WoundsDocument15 pagesStab WoundspreveennaNo ratings yet
- Surgitron Man EnglDocument8 pagesSurgitron Man EnglFernando CharryNo ratings yet
- Clarks Essential Guide To Clinical UltrasoundDocument77 pagesClarks Essential Guide To Clinical Ultrasoundrobertlinon0% (1)
- Amboss - Thoracic CavityDocument14 pagesAmboss - Thoracic CavityAllysahNo ratings yet
- Preparation For Children and Their Families: Voiding Cystourethrogram (VCUG)Document2 pagesPreparation For Children and Their Families: Voiding Cystourethrogram (VCUG)NataliaMaedyNo ratings yet
- Medical Language Instant Translator 6 Ed Edition Davi Ellen Chabner Full ChapterDocument67 pagesMedical Language Instant Translator 6 Ed Edition Davi Ellen Chabner Full Chaptermargaret.warner410100% (4)
- Principles and Safety Measures of Electrosurgery in LaparosDocument10 pagesPrinciples and Safety Measures of Electrosurgery in LaparosDuy HoàngNo ratings yet
- Git Radiology and ImagingDocument4 pagesGit Radiology and Imagingoddone_outNo ratings yet