You might also like
- Infectious Diseases RlsDocument54 pagesInfectious Diseases RlsA G I T ONo ratings yet
- INTERPRETATION OF Widal Test PDFDocument18 pagesINTERPRETATION OF Widal Test PDFstrawberry pieNo ratings yet
- COVID-19 Home & Long COVID Care by Sri Lankan GPsDocument26 pagesCOVID-19 Home & Long COVID Care by Sri Lankan GPsDineshani SirisenaNo ratings yet
- Dengue Fever Viruses: Causes, Symptoms, and TreatmentDocument4 pagesDengue Fever Viruses: Causes, Symptoms, and TreatmentDanis WaraNo ratings yet
- Publishing Case Reports: 8 Tips for SuccessDocument48 pagesPublishing Case Reports: 8 Tips for Successsryh2012No ratings yet
- Care of Pediatric Patients During COVID-19 Pandemic-04042020Document60 pagesCare of Pediatric Patients During COVID-19 Pandemic-04042020Florin StanciuNo ratings yet
- Manage Seasonal FluDocument7 pagesManage Seasonal FluAJEET KUMAR PANDEYNo ratings yet
- Emergency MedDocument4 pagesEmergency MedbencleeseNo ratings yet
- DIsaster Management in Pandemic EraDocument40 pagesDIsaster Management in Pandemic Erahandrian rahmanNo ratings yet
- Self Correcting ScienceDocument51 pagesSelf Correcting ScienceChristopher RossNo ratings yet
- Intra-Uterine and Perinatal InfectionDocument72 pagesIntra-Uterine and Perinatal InfectionsabrinaNo ratings yet
- Journal Reading ParuDocument53 pagesJournal Reading ParuDaniel IvanNo ratings yet
- TB-HIV Private PhysiciansDocument66 pagesTB-HIV Private PhysiciansZulhelmiNo ratings yet
- Febrile NeutropeniaDocument35 pagesFebrile NeutropeniaYogesh ShindeNo ratings yet
- SWINE FINAL Update An Indain PrespectiveDocument92 pagesSWINE FINAL Update An Indain PrespectiveperfectdocNo ratings yet
- Covid 19 ResidentsDocument64 pagesCovid 19 ResidentsJyotisai karNo ratings yet
- Hiv Seminar 2019Document49 pagesHiv Seminar 2019clarice_condeno100% (1)
- Typhoid and Paratyphoid Fever Public Health PlanDocument16 pagesTyphoid and Paratyphoid Fever Public Health PlanBayu Surya DanaNo ratings yet
- Diagnostic Testing For Community-Acquired Pneumonia (CAP) and InfluenzaDocument48 pagesDiagnostic Testing For Community-Acquired Pneumonia (CAP) and InfluenzaKartika RezkyNo ratings yet
- Macklon Covid Guidelines Webinar 25 May VersionDocument37 pagesMacklon Covid Guidelines Webinar 25 May VersionThuy Trang Nguyen ThiNo ratings yet
- Annotated-Tuberculosis PresentationDocument42 pagesAnnotated-Tuberculosis PresentationAnna mae AaronNo ratings yet
- Wa0004.Document17 pagesWa0004.Phoenix ParkerNo ratings yet
- Typhoid Fever Journal ArticleDocument5 pagesTyphoid Fever Journal ArticleDiana MargaretaNo ratings yet
- KMU CHN-LLL Final 2022Document20 pagesKMU CHN-LLL Final 2022AamirNo ratings yet
- Protect Yourself from Legionnaires' Disease: The Waterborne Illness That Continues to Kill and HarmFrom EverandProtect Yourself from Legionnaires' Disease: The Waterborne Illness That Continues to Kill and HarmNo ratings yet
- Facts About h1n1 InfluenzaDocument20 pagesFacts About h1n1 InfluenzaSureshkumar ManoharanNo ratings yet
- Covid-19 Primer 3-30-20Document100 pagesCovid-19 Primer 3-30-20Rodrigo LazoNo ratings yet
- Case #3 Pulmonary TBDocument3 pagesCase #3 Pulmonary TBje-ann catedralNo ratings yet
- MKSAP 16 - Infectious DiseaseDocument340 pagesMKSAP 16 - Infectious DiseaseBacanator75% (4)
- Halodoc Webinar On COVID 2020-03-21 V 0.4Document75 pagesHalodoc Webinar On COVID 2020-03-21 V 0.4Gabriella NelwanNo ratings yet
- Muhimbili COVID SummaryDocument7 pagesMuhimbili COVID SummaryMeNo ratings yet
- Cme On TuberclosisDocument12 pagesCme On TuberclosisOdulusi DanielNo ratings yet
- Review of Communicable DIsease NursingDocument252 pagesReview of Communicable DIsease NursingRodelyn DariaNo ratings yet
- Covid 19 Guidelines April 2021Document42 pagesCovid 19 Guidelines April 2021K.sushmaNo ratings yet
- What Is Hepatitis ?Document30 pagesWhat Is Hepatitis ?kazulamaNo ratings yet
- Hiv Dcmiii 2Document36 pagesHiv Dcmiii 2Mutegeki AdolfNo ratings yet
- Causes, Signs and Symptoms of Dengue Fever and Typhoid FeverDocument24 pagesCauses, Signs and Symptoms of Dengue Fever and Typhoid FeverrefkyjuliandriNo ratings yet
- Tuberculosis Research Paper ExampleDocument4 pagesTuberculosis Research Paper Exampled1fytyt1man3100% (1)
- Tuberculosis: Angeles University FoundationDocument10 pagesTuberculosis: Angeles University FoundationBob Joyce Dela PeñaNo ratings yet
- Dr. Sanjeev GuptaDocument73 pagesDr. Sanjeev Guptadrsanjeev15No ratings yet
- TEACHING KEY - CASES 11 - 15 (Dec. 7 Session)Document7 pagesTEACHING KEY - CASES 11 - 15 (Dec. 7 Session)Kishwar BasithNo ratings yet
- Acquired Immune Deficiency Syndrome or Acquired Immunodeficiency Syndrome (AIDS) Is A Disease of The Human Immune System Caused byDocument7 pagesAcquired Immune Deficiency Syndrome or Acquired Immunodeficiency Syndrome (AIDS) Is A Disease of The Human Immune System Caused byAdrian MallarNo ratings yet
- Mindoro child with recurrent fever, chills, sweating has malariaDocument16 pagesMindoro child with recurrent fever, chills, sweating has malariaJiezl Abellano Afinidad100% (2)
- Principles of Epidemic Outbreak InvestigationDocument46 pagesPrinciples of Epidemic Outbreak Investigationkuchie ranksNo ratings yet
- Tropmed - Lecture 4Document78 pagesTropmed - Lecture 4VerarisnaNo ratings yet
- CAD - EBM September 2020 EditionDocument17 pagesCAD - EBM September 2020 EditionNaga Venkatamanoj Kumar PakalapatiNo ratings yet
- Presentation By:-Capt Narendra Sarlam MH GwaliorDocument66 pagesPresentation By:-Capt Narendra Sarlam MH Gwalioryash shrivastavaNo ratings yet
- C3.5 (C3.4) PEP and Needle Stick InjuryDocument8 pagesC3.5 (C3.4) PEP and Needle Stick Injuryvasthare phcNo ratings yet
- Covid 19Document21 pagesCovid 19Jixon GeorgeNo ratings yet
- 2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFDocument4 pages2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFteteh_thikeuNo ratings yet
- Typhoid Fever Diagnosis and TreatmentDocument7 pagesTyphoid Fever Diagnosis and Treatmentfitrian amwaalunNo ratings yet
- Final Infectious Pe - 1-EditDocument59 pagesFinal Infectious Pe - 1-EditAhmad SobihNo ratings yet
- Polio Investigation GuidelineDocument11 pagesPolio Investigation Guidelineaikohama89No ratings yet
- Pathology I Review 10Document30 pagesPathology I Review 10i_areinamoNo ratings yet
- DAY 2 RH ABOHIVAIDSECTOPICHMOLE Etc.Document29 pagesDAY 2 RH ABOHIVAIDSECTOPICHMOLE Etc.Marga WreatheNo ratings yet
- Infection PICU 1Document33 pagesInfection PICU 1Mohamed ElgayarNo ratings yet
- Class AidsDocument45 pagesClass AidsSrinivas KasiNo ratings yet
- Antiretroviral Therapy: Awlachew Firde (S.Pharmacist)Document40 pagesAntiretroviral Therapy: Awlachew Firde (S.Pharmacist)wedajoyonas50No ratings yet
- TB and HIVDocument43 pagesTB and HIVNational Press Foundation100% (1)
- Bicycle BasicsDocument3 pagesBicycle BasicsJatin GulatiNo ratings yet
- Motorbike DesignDocument4 pagesMotorbike DesignJatin GulatiNo ratings yet
- Software Design BasicsDocument4 pagesSoftware Design BasicsJatin GulatiNo ratings yet
- Types of MiningDocument3 pagesTypes of MiningJatin GulatiNo ratings yet
- Radiator BasicsDocument3 pagesRadiator BasicsJatin GulatiNo ratings yet
- Corona Presentation 3Document19 pagesCorona Presentation 3Jatin GulatiNo ratings yet
- Chapter 38: MERGE 123: 123 Examples 123Document3 pagesChapter 38: MERGE 123: 123 Examples 123Jatin GulatiNo ratings yet
- Implicit JoinsDocument6 pagesImplicit JoinsJatin GulatiNo ratings yet
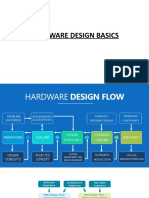
- Hardware Design BasicsDocument4 pagesHardware Design BasicsJatin GulatiNo ratings yet
- Chapter 1: Getting Started With SQL: RemarksDocument3 pagesChapter 1: Getting Started With SQL: RemarksJatin GulatiNo ratings yet
- Sample Data 13 Query 13 Results 14 Explanation 14 Chapter 6: Clean Code in SQL 15Document5 pagesSample Data 13 Query 13 Results 14 Explanation 14 Chapter 6: Clean Code in SQL 15Jatin GulatiNo ratings yet
- SQL Server 69Document3 pagesSQL Server 69Jatin GulatiNo ratings yet
- Hortonworks Do Hadoop: Successfully EverywhereDocument1 pageHortonworks Do Hadoop: Successfully EverywhereJatin GulatiNo ratings yet
- Chapter 53: Subqueries 176: Remarks 176 Examples 176Document3 pagesChapter 53: Subqueries 176: Remarks 176 Examples 176Jatin GulatiNo ratings yet
- 436Document1 page436Jatin GulatiNo ratings yet
- 64 I P - C XI: OutputDocument1 page64 I P - C XI: OutputJatin GulatiNo ratings yet
- JKLDocument2,419 pagesJKLJatin GulatiNo ratings yet
- Mathematical Decision Making: Predictive Models and OptimizationDocument1 pageMathematical Decision Making: Predictive Models and OptimizationJatin GulatiNo ratings yet
- 4.1.2 Lists Are Mutable: IST PerationsDocument1 page4.1.2 Lists Are Mutable: IST PerationsJatin GulatiNo ratings yet
- 4.2.2 Repetition: 58 I P - C XIDocument1 page4.2.2 Repetition: 58 I P - C XIJatin GulatiNo ratings yet
- Orking With Ists and IctionariesDocument1 pageOrking With Ists and IctionariesJatin GulatiNo ratings yet
- Visitor Arrivals Annual SummaryDocument12 pagesVisitor Arrivals Annual SummaryJatin GulatiNo ratings yet
- 4.2.2 Repetition: 58 I P - C XIDocument1 page4.2.2 Repetition: 58 I P - C XIJatin GulatiNo ratings yet
- 56 I P - C XI: 4.1.1 Accessing Elements in A ListDocument1 page56 I P - C XI: 4.1.1 Accessing Elements in A ListJatin GulatiNo ratings yet
- Resume: OBJECTIVE: To Secure The Challenging Position Where I Can Apply My Technical SkillsDocument1 pageResume: OBJECTIVE: To Secure The Challenging Position Where I Can Apply My Technical SkillsJatin GulatiNo ratings yet
- Visitor Arrivals Annual SummaryDocument12 pagesVisitor Arrivals Annual SummaryJatin GulatiNo ratings yet
- 56 I P - C XI: 4.1.1 Accessing Elements in A ListDocument1 page56 I P - C XI: 4.1.1 Accessing Elements in A ListJatin GulatiNo ratings yet
- Visitor Arrivals Annual SummaryDocument12 pagesVisitor Arrivals Annual SummaryJatin GulatiNo ratings yet
- A New Typology of Augmented Reality Applications: Jean-Marie Normand, Myriam Servières, Guillaume MoreauDocument9 pagesA New Typology of Augmented Reality Applications: Jean-Marie Normand, Myriam Servières, Guillaume MoreauJatin GulatiNo ratings yet
- Effectiveness of Mesotherapy On Body Contouring: BackgroundDocument7 pagesEffectiveness of Mesotherapy On Body Contouring: BackgroundNita Dewi NNo ratings yet
- Case Study 01 Workplace Violence - Mariam WakedDocument1 pageCase Study 01 Workplace Violence - Mariam WakedMariam WakedNo ratings yet
- ER Diagram ExerciseDocument2 pagesER Diagram ExerciseFarhana NaziraNo ratings yet
- Exerciții Pe TEXT 2Document27 pagesExerciții Pe TEXT 2Balanean TatianaNo ratings yet
- CGM Comparison For People With Insulin Treated Research July 2023Document11 pagesCGM Comparison For People With Insulin Treated Research July 2023shahirahNo ratings yet
- Ipsg 2017Document41 pagesIpsg 2017hum JavedNo ratings yet
- Depression and Mental Wellbeing in People Affected by Leprosy in Southern NepalDocument9 pagesDepression and Mental Wellbeing in People Affected by Leprosy in Southern NepalMedNo ratings yet
- The Effects of Caffeine and Expectancy On Attention and MemoryDocument10 pagesThe Effects of Caffeine and Expectancy On Attention and MemoryMunkhtsolmon GantulgaNo ratings yet
- The Baltimore SunDocument21 pagesThe Baltimore SunАгент ГусьNo ratings yet
- 10 Medicinal Plants Approved by The Department of HealthDocument4 pages10 Medicinal Plants Approved by The Department of HealthASHLEY NICOLE JACINTONo ratings yet
- Module 1Document26 pagesModule 1priya malikNo ratings yet
- Identification of Aerobic Pathogenic Bacteria Isolated From Ready-to-Eat Cakes Sold in Traditional Markets in Manado CityDocument3 pagesIdentification of Aerobic Pathogenic Bacteria Isolated From Ready-to-Eat Cakes Sold in Traditional Markets in Manado CityVenita NapitNo ratings yet
- Ecl SW Iso45001Document92 pagesEcl SW Iso45001Meghanath LalemmaNo ratings yet
- COBADocument222 pagesCOBArendiNo ratings yet
- Lauren Makosky ResumeDocument2 pagesLauren Makosky Resumeapi-634419348No ratings yet
- Women EmpowermentDocument15 pagesWomen EmpowermentMaya DevikaNo ratings yet
- Igcse Biology Concepts Revision Chapter 1 To 8Document9 pagesIgcse Biology Concepts Revision Chapter 1 To 8naduniNo ratings yet
- Test Bank For Burtons Microbiology For The Health Sciences 9 North Americanth Edition Paul G EngelkirkDocument10 pagesTest Bank For Burtons Microbiology For The Health Sciences 9 North Americanth Edition Paul G Engelkirkraphaelsophiep9f9100% (22)
- Details Received From Collectorate - Excellent Dedicated Work - During Pandemic COVID - 19Document2 pagesDetails Received From Collectorate - Excellent Dedicated Work - During Pandemic COVID - 19Vimal kumarNo ratings yet
- Unitati Certificare A5Document2 pagesUnitati Certificare A5enaionNo ratings yet
- Outcomes Before and After Total Knee Arthroplasty Compared To Healthy AdultsDocument20 pagesOutcomes Before and After Total Knee Arthroplasty Compared To Healthy AdultsFirdaus Septhy ArdhyanNo ratings yet
- Bahan Kuliah MHM Beginning BioethicsDocument80 pagesBahan Kuliah MHM Beginning BioethicsKlarasita WibowoNo ratings yet
- Denah Mixed Use LT 3 &4Document1 pageDenah Mixed Use LT 3 &4Jennifer MadenNo ratings yet
- Galway All Products Price ListDocument3 pagesGalway All Products Price ListRishikesh Kumar Ray madhaipurNo ratings yet
- Benefits of Intermittent FastingDocument3 pagesBenefits of Intermittent FastingSaurabh PandeyNo ratings yet
- Pianakafinal Sa Lahatt RyannDocument14 pagesPianakafinal Sa Lahatt RyannPaul IglesiasNo ratings yet
- PhobiasDocument4 pagesPhobiasOti VuraNo ratings yet
- Cagri Karaciklar Fragility Fractures Presentation PDFDocument15 pagesCagri Karaciklar Fragility Fractures Presentation PDFÇağrıNo ratings yet
- Depression Associated With Dementia With Lewy Bodies (DLB) and The Effect of SomatotherapyDocument6 pagesDepression Associated With Dementia With Lewy Bodies (DLB) and The Effect of SomatotherapyRaluca ElenaNo ratings yet
- CWTS ProposalDocument5 pagesCWTS ProposalAllana de CastroNo ratings yet