You might also like
- Prometric Pharmacy MCQs (Solved)Document45 pagesPrometric Pharmacy MCQs (Solved)cuami84% (45)
- Case Study On CVADocument22 pagesCase Study On CVAAgronaSlaughter100% (3)
- The Effect by Lucy PrebbleDocument110 pagesThe Effect by Lucy Prebble6jbrsvkqvk100% (3)
- Concept Map Cystic FibrosisDocument1 pageConcept Map Cystic FibrosisAnne B. Buenvenida100% (1)
- EMT Course NotesDocument88 pagesEMT Course NotesHunter RobertsNo ratings yet
- MR 23 Oktober 2019Document17 pagesMR 23 Oktober 2019yantiNo ratings yet
- Case I: Name: Mrs. M Age: 31 Y.O. Address:Narmada Admitted: 26 September, 2019 MR Number: 044656Document10 pagesCase I: Name: Mrs. M Age: 31 Y.O. Address:Narmada Admitted: 26 September, 2019 MR Number: 044656Inatul AuliaNo ratings yet
- Morning Report: Supervisor: Dr. Edi Prasetyo Wibowo, SP - OGDocument19 pagesMorning Report: Supervisor: Dr. Edi Prasetyo Wibowo, SP - OGGustini WidiyaningsihNo ratings yet
- MR Obgyn KPD Sabtu, 8 AprilDocument6 pagesMR Obgyn KPD Sabtu, 8 AprilRdindaaNo ratings yet
- Morning Report: Supervisor: Dr. Gede Made Punarbhawa, SP - OG (K)Document13 pagesMorning Report: Supervisor: Dr. Gede Made Punarbhawa, SP - OG (K)Tannia Rizkyka IrawanNo ratings yet
- Morning Report: Supervisor: Dr. Ario Danianto, SP - OGDocument11 pagesMorning Report: Supervisor: Dr. Ario Danianto, SP - OGGustini WidiyaningsihNo ratings yet
- Supervisor: Dr. Juliawan, SP - OG Medical Students:: Morning ReportDocument10 pagesSupervisor: Dr. Juliawan, SP - OG Medical Students:: Morning ReportZainul MuttaqinNo ratings yet
- Case 3: - Name: Mrs. M - Age: 23 Yo - Address: Lingsar, Lombok Barat - Admitted: 6 July 2017 - RM: 594222Document4 pagesCase 3: - Name: Mrs. M - Age: 23 Yo - Address: Lingsar, Lombok Barat - Admitted: 6 July 2017 - RM: 594222Ahmad HavizNo ratings yet
- Morning Report: Supervisor: Dr. Made Mahayasa, SP - OGDocument5 pagesMorning Report: Supervisor: Dr. Made Mahayasa, SP - OGZainul MuttaqinNo ratings yet
- Morning Report 5 April 2016 (PROM)Document64 pagesMorning Report 5 April 2016 (PROM)Brian DepamedeNo ratings yet
- Morning Report: Supervisor: DRDocument22 pagesMorning Report: Supervisor: DRAhmad HavizNo ratings yet
- MR 22-05-2019 NewDocument8 pagesMR 22-05-2019 NewFafan upinNo ratings yet
- MR 24-05-2019Document12 pagesMR 24-05-2019Fafan upinNo ratings yet
- Morning Report: 27 OCTOBER, 2019Document11 pagesMorning Report: 27 OCTOBER, 2019yantiNo ratings yet
- MR 25 Oktober 2017Document13 pagesMR 25 Oktober 2017Sri RohmayanaNo ratings yet
- Tidak Ada Pertanyaan Yang SalahDocument13 pagesTidak Ada Pertanyaan Yang SalahTannia Rizkyka IrawanNo ratings yet
- Case 3 29-6-2016Document8 pagesCase 3 29-6-2016Faishal AkbarNo ratings yet
- Morning Report August, 4 20168: Supervisor: Dr. Sp. OG DM Jaga: Verga, Hani, Nisa, SilminaDocument11 pagesMorning Report August, 4 20168: Supervisor: Dr. Sp. OG DM Jaga: Verga, Hani, Nisa, SilminaYeyen NadianNo ratings yet
- MR 18 Nov 2018 CPDDocument16 pagesMR 18 Nov 2018 CPDKuran AtikaNo ratings yet
- Agnes MR 21-12-2017 Peb Dan KPDDocument23 pagesAgnes MR 21-12-2017 Peb Dan KPDGustini WidiyaningsihNo ratings yet
- MR Minus GambarDocument26 pagesMR Minus GambarmarjoranovaNo ratings yet
- Morning Report 251017Document27 pagesMorning Report 251017Dewi Rabiatul AkhzamiNo ratings yet
- 4 7 17 Post Date PakaiDocument8 pages4 7 17 Post Date PakaiAhmad HavizNo ratings yet
- 04-07-12 Eklampsia PuerperiumDocument8 pages04-07-12 Eklampsia PuerperiumZainul MuttaqinNo ratings yet
- MR 04 May 2019Document17 pagesMR 04 May 2019Fafan upinNo ratings yet
- July 8, 2016: Supervisor: Dr. Juliawan SP - OG Medical Students: Ayu, Dimas, Siti ShabrinaDocument41 pagesJuly 8, 2016: Supervisor: Dr. Juliawan SP - OG Medical Students: Ayu, Dimas, Siti ShabrinaIka Putri YulianiNo ratings yet
- Case Kehamilan Ektopik TergangguDocument17 pagesCase Kehamilan Ektopik TergangguwilliamNo ratings yet
- GemelliDocument4 pagesGemelliDarling Sevenfoldism SynysterNo ratings yet
- Morning Report 28 JuniDocument17 pagesMorning Report 28 JuniAhsanuddin Al AnsoriNo ratings yet
- Ny. H - 34 Yo - Seteluk, Western of Sumbawa - Islam - G1P0A0L0 A/S/L/IU With Neglected 2nd Stage of LaborDocument5 pagesNy. H - 34 Yo - Seteluk, Western of Sumbawa - Islam - G1P0A0L0 A/S/L/IU With Neglected 2nd Stage of LaborZainul MuttaqinNo ratings yet
- Morning Report: Supervisor: Dr. Windiana Rambu, SP - OGDocument12 pagesMorning Report: Supervisor: Dr. Windiana Rambu, SP - OGGustini WidiyaningsihNo ratings yet
- MR 20 Desember KPD + AbortusDocument15 pagesMR 20 Desember KPD + AbortusNetii FarhatiNo ratings yet
- Morning Report: Physician in ChargeDocument21 pagesMorning Report: Physician in ChargePHOENIX LUNANo ratings yet
- Jepretan Layar 2021-01-27 Pada 21.01.47Document13 pagesJepretan Layar 2021-01-27 Pada 21.01.47nadyaNo ratings yet
- Pre AmnionreductionDocument5 pagesPre AmnionreductionNovhy GanggutNo ratings yet
- 4 7 17 Post DateDocument11 pages4 7 17 Post DateAhmad HavizNo ratings yet
- Morning Report: Mataram University HospitalDocument44 pagesMorning Report: Mataram University HospitaldellaNo ratings yet
- 11-08-2012 Kala II Kasep + CPD + SCDocument5 pages11-08-2012 Kala II Kasep + CPD + SCZainul MuttaqinNo ratings yet
- Morning Report: Case Resume Normal Labor - Pathology LaborDocument7 pagesMorning Report: Case Resume Normal Labor - Pathology LabormelatiigdNo ratings yet
- Morning Report: Supervisor: Dr. H. Agus Thoriq, SP - OGDocument20 pagesMorning Report: Supervisor: Dr. H. Agus Thoriq, SP - OGIka Putri YulianiNo ratings yet
- Mapping ANC, B31 3 Agustus 20222Document3 pagesMapping ANC, B31 3 Agustus 20222Handoyo SasongkoNo ratings yet
- Morning Report 14 April 2016 (Anemia Berat)Document15 pagesMorning Report 14 April 2016 (Anemia Berat)Brian DepamedeNo ratings yet
- Active Phase of LaborDocument6 pagesActive Phase of LaborIda_Maryani94No ratings yet
- Morning Report AbortusDocument6 pagesMorning Report AbortusmelatiigdNo ratings yet
- Morning Report 1 September 2014Document11 pagesMorning Report 1 September 2014Arie Krisnayanti Ida AyuNo ratings yet
- Case Conference Sunday Night Shift, October 14 2018Document26 pagesCase Conference Sunday Night Shift, October 14 2018Hendra WardhanaNo ratings yet
- Laporan Kasus KJDRDocument7 pagesLaporan Kasus KJDRPutra MahautamaNo ratings yet
- REV MR Tama Medcon Hiperglicemia State Perioperative 131220Document11 pagesREV MR Tama Medcon Hiperglicemia State Perioperative 131220Lilik AndayatiNo ratings yet
- Morning Report 09 Mei 2016 (Kista Ovarium)Document12 pagesMorning Report 09 Mei 2016 (Kista Ovarium)Brian DepamedeNo ratings yet
- 11-11-22 LT 2 and GDocument22 pages11-11-22 LT 2 and GJhon WickNo ratings yet
- Morning Report 12 July 2014: SPV: Dr. Edi P.W, Spog DM: Vendi, Rian, Dayu, Ayu, NurulDocument8 pagesMorning Report 12 July 2014: SPV: Dr. Edi P.W, Spog DM: Vendi, Rian, Dayu, Ayu, NurulEzraNo ratings yet
- ChendrawatiDocument11 pagesChendrawatiGina ArianiNo ratings yet
- Morning Report: Supervisor: Dr. Punarbawa, SP - OGDocument25 pagesMorning Report: Supervisor: Dr. Punarbawa, SP - OGRdindaaNo ratings yet
- AYU - CKD+DVT Left ArmDocument25 pagesAYU - CKD+DVT Left ArmIka AyuNo ratings yet
- PreskasDocument52 pagesPreskasamirah sinumNo ratings yet
- Case Presentation: Appaji, Benita Imd Clerk 02-09-2011Document41 pagesCase Presentation: Appaji, Benita Imd Clerk 02-09-2011Benita Janet AppajiNo ratings yet
- Partus NormalDocument13 pagesPartus NormalGraham Allen ShowNo ratings yet
- No Sub Bagian Lama Baru Pulang Pindah JMLDocument32 pagesNo Sub Bagian Lama Baru Pulang Pindah JMLkavi_1985No ratings yet
- MR RS Unram 11 - 03 - 2021Document30 pagesMR RS Unram 11 - 03 - 2021Nia TazmaniaNo ratings yet
- MR 22-05-2019 NewDocument8 pagesMR 22-05-2019 NewFafan upinNo ratings yet
- MR 24-05-2019Document12 pagesMR 24-05-2019Fafan upinNo ratings yet
- MR 04 May 2019Document17 pagesMR 04 May 2019Fafan upinNo ratings yet
- Rekapan Data ExelDocument28 pagesRekapan Data ExelFafan upinNo ratings yet
- MR Ny. NoniDocument5 pagesMR Ny. NoniFafan upinNo ratings yet
- Dapus SemproDocument6 pagesDapus SemproFafan upinNo ratings yet
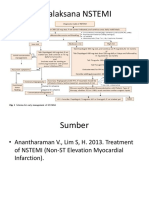
- Tatalaksana NSTEMIDocument2 pagesTatalaksana NSTEMIFafan upinNo ratings yet
- Reumatoid AtritisDocument6 pagesReumatoid AtritisFafan upinNo ratings yet
- Medicine Admitting Conference: University of Santo Tomas Faculty of Medicine and SurgeryDocument70 pagesMedicine Admitting Conference: University of Santo Tomas Faculty of Medicine and SurgerySTEPHANIE TANNo ratings yet
- BIOLOGY Form 5 Chapter 1 TransportDocument42 pagesBIOLOGY Form 5 Chapter 1 TransportShephard Png91% (95)
- GMDSS Exam Schedule For Year 2022Document7 pagesGMDSS Exam Schedule For Year 2022Mani ThapaNo ratings yet
- List of Common Disabilities !Document1 pageList of Common Disabilities !Shannon Elaine SmithNo ratings yet
- Vaginitis: Dr. Zienab Halem Faculty of Pharmacy SCUDocument25 pagesVaginitis: Dr. Zienab Halem Faculty of Pharmacy SCUshona SharupaniNo ratings yet
- TEJASWINIDocument8 pagesTEJASWINIAyush JamwalNo ratings yet
- Mark Scheme (FINAL) : Summer 2018Document19 pagesMark Scheme (FINAL) : Summer 2018Ammatul AyeshaNo ratings yet
- Multiple Choice Questions - Answers: 1. A B C DDocument5 pagesMultiple Choice Questions - Answers: 1. A B C Dsafa_sabaNo ratings yet
- Antibacterial Mechanism of Lactic Acid On Physiological andDocument6 pagesAntibacterial Mechanism of Lactic Acid On Physiological andlox standardNo ratings yet
- Benefits of Prana Mudra and How To Do It by Dr. Himani Bisht - PharmEasy BlogDocument7 pagesBenefits of Prana Mudra and How To Do It by Dr. Himani Bisht - PharmEasy BlogDanaNo ratings yet
- Perez 2007Document8 pagesPerez 2007SNo ratings yet
- Zoonoses and Emerging Livestock Systems (ZELS) Supplementary Research Projects 2019-2021Document7 pagesZoonoses and Emerging Livestock Systems (ZELS) Supplementary Research Projects 2019-2021dukegarrikNo ratings yet
- Research Proposal Group 2Document30 pagesResearch Proposal Group 2Anthony PelayoNo ratings yet
- Anatomy Module 17Document23 pagesAnatomy Module 17JayR MendonesNo ratings yet
- Analysis of Heavy Metals in Vegetable and Agricultural Soil Samples in Gemikonagi and Dipkarpaz (North Cyprus)Document82 pagesAnalysis of Heavy Metals in Vegetable and Agricultural Soil Samples in Gemikonagi and Dipkarpaz (North Cyprus)Ibrahim MoserayNo ratings yet
- Pattern and Causes of Tooth Extraction in Patients Reporting To A Teaching Dental HospitalDocument6 pagesPattern and Causes of Tooth Extraction in Patients Reporting To A Teaching Dental HospitalAnye PutriNo ratings yet
- BSP Treatment Flow Chart 16 For ScreenDocument2 pagesBSP Treatment Flow Chart 16 For ScreenshahadNo ratings yet
- Paarambariya MaruthuvamDocument1 pagePaarambariya MaruthuvamAnonymous kCrS4NduNo ratings yet
- Who Shall Be Considered As Having Community-Acquired Pneumonia?Document4 pagesWho Shall Be Considered As Having Community-Acquired Pneumonia?Kristine Jade OdtujanNo ratings yet
- Furcation InvolvementDocument39 pagesFurcation InvolvementShaju Jacob PNo ratings yet
- Debate at Home: Tentative Scientific ProgramDocument10 pagesDebate at Home: Tentative Scientific ProgramManish SharmaNo ratings yet
- Subjective:: Assessment Nursing Diagnosis Planning Interventi ONS Rationale EvaluationDocument2 pagesSubjective:: Assessment Nursing Diagnosis Planning Interventi ONS Rationale EvaluationCuttie Anne GalangNo ratings yet
- TLE Module 4 and Quiz Naa Sa Tumoy.Document5 pagesTLE Module 4 and Quiz Naa Sa Tumoy.franciscoNo ratings yet
- 高等学校研究生英语系列教材 综合教程(上)主编熊海虹 教学课件 Unit 1Document129 pages高等学校研究生英语系列教材 综合教程(上)主编熊海虹 教学课件 Unit 1yvaineNo ratings yet
- Idiopathic Osteosclerosis of The Jaws: Panoramic Radiographic and Computed Tomographic FindingsDocument5 pagesIdiopathic Osteosclerosis of The Jaws: Panoramic Radiographic and Computed Tomographic FindingslauNo ratings yet