You might also like
- Modafinil. A Legit Smart Pill That Improves Cognitive FunctionFrom EverandModafinil. A Legit Smart Pill That Improves Cognitive FunctionRating: 5 out of 5 stars5/5 (1)
- Understanding CNS DepressantsDocument49 pagesUnderstanding CNS DepressantsMirza Shaharyar BaigNo ratings yet
- Pharmacology of The Central Nervous System-1Document163 pagesPharmacology of The Central Nervous System-1Gølà Sèèñàà–baale irraaNo ratings yet
- Penyalahgunaan ObatDocument26 pagesPenyalahgunaan Obatvinna iasyaNo ratings yet
- Mohammad Ryad Goulvaden 5 Year, Faculty of PharmacyDocument40 pagesMohammad Ryad Goulvaden 5 Year, Faculty of PharmacypharmryadNo ratings yet
- Sedative HypnoticsDocument33 pagesSedative HypnoticsIkram HamacheNo ratings yet
- WEEK 6 7-CNS Medications StudentDocument83 pagesWEEK 6 7-CNS Medications Studentx8jdbj5gphNo ratings yet
- Drugs, Addiction, and RewardDocument71 pagesDrugs, Addiction, and RewardBoemo BolaaneNo ratings yet
- Effects and Side Effects of Psychoactive DrugsDocument14 pagesEffects and Side Effects of Psychoactive Drugsathena villaNo ratings yet
- Drugs Affecting CNS & PNSDocument131 pagesDrugs Affecting CNS & PNSMj Briones100% (1)
- Pharmacology in PsychiatryDocument33 pagesPharmacology in PsychiatryKatrina PonceNo ratings yet
- 7 - Anxiolytics-Sedatives-HypnoticsDocument46 pages7 - Anxiolytics-Sedatives-HypnoticsHadeelNo ratings yet
- Psychotropic Drugs: Bryan Mae H. DegorioDocument65 pagesPsychotropic Drugs: Bryan Mae H. DegorioBryan Mae H. Degorio100% (2)
- Sedative HypnoticsDocument39 pagesSedative HypnoticsFatima ShaukatNo ratings yet
- Anxiolytics Sedatives Hypnotics Pharm 3Document38 pagesAnxiolytics Sedatives Hypnotics Pharm 3Peter Harris100% (1)
- CHAPTER 22 Psychotherapeutic AgentsDocument4 pagesCHAPTER 22 Psychotherapeutic AgentsJewel SantosNo ratings yet
- NSTP Reviewer MidtermsDocument14 pagesNSTP Reviewer MidtermsSara AlbinaNo ratings yet
- Pharmacology CNS DepressantDocument31 pagesPharmacology CNS DepressantQueenie PuzonNo ratings yet
- 6) 5th Semester - Sedative Hypnotics and Antianxiety DrugsDocument34 pages6) 5th Semester - Sedative Hypnotics and Antianxiety DrugsFizza ImamNo ratings yet
- Introduction Classification Benzodiazepines BarbituratesDocument15 pagesIntroduction Classification Benzodiazepines BarbituratesVijetha RaiNo ratings yet
- Types and Uses of Anti-Anxiety DrugsDocument39 pagesTypes and Uses of Anti-Anxiety DrugsArkene LevyNo ratings yet
- Cns PharmacologyDocument51 pagesCns PharmacologyAnasAbdelaNo ratings yet
- Anxiolytic, Sedative-Hypnotic DrugsDocument39 pagesAnxiolytic, Sedative-Hypnotic DrugsNina100% (1)
- AnxiolyticsDocument23 pagesAnxiolyticsNalafNo ratings yet
- AnxietyDocument6 pagesAnxietyMasa MasaNo ratings yet
- نسخة Antidepressants for Lab. StudentsDocument64 pagesنسخة Antidepressants for Lab. Studentsنوف الحربي.No ratings yet
- Drug PresentationDocument32 pagesDrug PresentationManisha ShakyaNo ratings yet
- Anxiolytics, Sedative & Hypnotic DrugsDocument22 pagesAnxiolytics, Sedative & Hypnotic DrugsPh Hany MohamedNo ratings yet
- 1 Medicatia SNCDocument29 pages1 Medicatia SNCMiruna-CristianaBirtuNo ratings yet
- Cns Depressants Sedative-Hypnotic Drugs: Dr. Hiwa K. Saaed, BSC, HD, Msc. PHDDocument42 pagesCns Depressants Sedative-Hypnotic Drugs: Dr. Hiwa K. Saaed, BSC, HD, Msc. PHDmiznahNo ratings yet
- Anxiolytic and Hypnotic DrugsDocument6 pagesAnxiolytic and Hypnotic DrugsFalah Dakka100% (2)
- Anti Anxiety DrugsDocument15 pagesAnti Anxiety DrugsMr. Psycho SamNo ratings yet
- PSYCHOPHARMACOLOGY HndoutDocument12 pagesPSYCHOPHARMACOLOGY HndoutMhae TabasaNo ratings yet
- 13 Psychiatric DRUGSDocument42 pages13 Psychiatric DRUGSPande Indra PremanaNo ratings yet
- Overview of Psychotropic DrugsDocument7 pagesOverview of Psychotropic Drugsnad101No ratings yet
- Unit 6 Drugs Acting On The CNS and PNSDocument43 pagesUnit 6 Drugs Acting On The CNS and PNSTherese Margarette SantiagoNo ratings yet
- Psychopharmacology Article StyleDocument9 pagesPsychopharmacology Article StyleLizethNo ratings yet
- PsychopharmacologyDocument31 pagesPsychopharmacologyɹǝʍdןnos100% (8)
- Psychopharmacology UCEBT Presentation Slides PDFDocument42 pagesPsychopharmacology UCEBT Presentation Slides PDFjay ar baybayNo ratings yet
- Typical Antipsychotic DrugsDocument4 pagesTypical Antipsychotic DrugsErika Blaire N. OlacaoNo ratings yet
- Drugs Acting On The CNSI: Unit 4 Week 5 Siti Ma'rufahDocument26 pagesDrugs Acting On The CNSI: Unit 4 Week 5 Siti Ma'rufahnur rachmad afandiNo ratings yet
- Neurotransmitters and Drugs ChartDocument6 pagesNeurotransmitters and Drugs ChartTammy Tam100% (5)
- AnxiolyticsDocument8 pagesAnxiolyticsHengky_FandriNo ratings yet
- Pharmacology of Sedative-HypnoticsDocument49 pagesPharmacology of Sedative-HypnoticsGeorge AbrahamNo ratings yet
- 2 - Substance Abuse - LAGDocument65 pages2 - Substance Abuse - LAGBritneyNo ratings yet
- Lecture 28 - 3rd Asessment - Sedatives, HypnoticsDocument32 pagesLecture 28 - 3rd Asessment - Sedatives, Hypnoticsapi-3703352100% (1)
- Sedative and Hypnotic DrugsDocument4 pagesSedative and Hypnotic DrugsSheila May AlipioNo ratings yet
- Treatment Day 1Document28 pagesTreatment Day 1api-433532127No ratings yet
- Drugs Acting On The CNS - 2Document41 pagesDrugs Acting On The CNS - 2Daniel OkakaNo ratings yet
- HBJHHBDocument29 pagesHBJHHBKYLE MITZIE SENGCONo ratings yet
- Psychiatric Agents: By: Paula Rose Mae Cuario Evita Lalaine Del Mundo Dennis Ragudo Sheena ZarsueloDocument80 pagesPsychiatric Agents: By: Paula Rose Mae Cuario Evita Lalaine Del Mundo Dennis Ragudo Sheena ZarsueloDennis RagudoNo ratings yet
- Cns StimulantsDocument4 pagesCns StimulantsKienna GarciaNo ratings yet
- Psychotherapy Biomedical Techniques PresentationDocument92 pagesPsychotherapy Biomedical Techniques PresentationRhea Andrea UyNo ratings yet
- 911 Sedative-Hypnotics PDFDocument17 pages911 Sedative-Hypnotics PDFIkram HamacheNo ratings yet
- Use Cautiously in: History of suicide attempts or substance abuseDocument2 pagesUse Cautiously in: History of suicide attempts or substance abuseidullrufaidahNo ratings yet
- Related Learning Experience: NCM 105 Psychiatric NursingDocument18 pagesRelated Learning Experience: NCM 105 Psychiatric NursingDyanne BautistaNo ratings yet
- Human Health & Disease Chapter on DrugsDocument14 pagesHuman Health & Disease Chapter on DrugsNikhil BijuNo ratings yet
- Psychotro Pic Drugs: Sedative and Hypnotic DrugsDocument15 pagesPsychotro Pic Drugs: Sedative and Hypnotic DrugsBajoijoi Ordiz-sandro EncisaNo ratings yet
- Anti PsychoticsDocument34 pagesAnti Psychotics88AKKNo ratings yet
- OFLOXACINDocument3 pagesOFLOXACINfayrouz fathiNo ratings yet
- Streptomycin use and monitoring in MDR-TBDocument3 pagesStreptomycin use and monitoring in MDR-TBfayrouz fathiNo ratings yet
- MOXIFLOXACIN MonographDocument3 pagesMOXIFLOXACIN Monographfayrouz fathiNo ratings yet
- MEROPENEM MonographDocument3 pagesMEROPENEM Monographfayrouz fathiNo ratings yet
- LINEZOLID MonographDocument3 pagesLINEZOLID Monographfayrouz fathiNo ratings yet
- LEVOFLOXACIN MonographDocument3 pagesLEVOFLOXACIN Monographfayrouz fathiNo ratings yet
- COPD - Chronic Objective Pulmonary DiseaseDocument22 pagesCOPD - Chronic Objective Pulmonary Diseasefayrouz fathiNo ratings yet
- HepatoprotectionDocument19 pagesHepatoprotectionfayrouz fathiNo ratings yet
- Effect of Liver Disease On PharmacokineticsDocument17 pagesEffect of Liver Disease On Pharmacokineticsfayrouz fathiNo ratings yet
- First Aid KitDocument15 pagesFirst Aid Kitdex adecNo ratings yet
- Manual Mta TemperaturaDocument2 pagesManual Mta TemperaturaChristian JacoboNo ratings yet
- MS6711 Data Mining Homework 1: 1.1 Implement K-Means Manually (8 PTS)Document6 pagesMS6711 Data Mining Homework 1: 1.1 Implement K-Means Manually (8 PTS)Yihan WangNo ratings yet
- Unit 5 - Lesson 1 - Understanding Hypothesis TestingDocument31 pagesUnit 5 - Lesson 1 - Understanding Hypothesis TestingJasper A. SANTIAGONo ratings yet
- Standardized Trade Types Fact SheetDocument2 pagesStandardized Trade Types Fact SheetRik100% (1)
- Pharmaceutical Stability The Science and RegulationsDocument32 pagesPharmaceutical Stability The Science and RegulationsMostofa Rubal100% (1)
- New Technique for Producing 3D Fabrics Using Conventional LoomDocument1 pageNew Technique for Producing 3D Fabrics Using Conventional LoomSujit GulhaneNo ratings yet
- Power Grid FailureDocument18 pagesPower Grid Failurechandra 798No ratings yet
- Practice Reading GraphsDocument4 pagesPractice Reading GraphsSharon TaylorNo ratings yet
- Social Engineering For Pentester PenTest - 02 - 2013Document81 pagesSocial Engineering For Pentester PenTest - 02 - 2013Black RainNo ratings yet
- Astm A710Document3 pagesAstm A710Cristian Otivo100% (1)
- Mil STD 882eDocument104 pagesMil STD 882ecihan dağNo ratings yet
- Probability Concepts and Random Variable - SMTA1402: Unit - IDocument105 pagesProbability Concepts and Random Variable - SMTA1402: Unit - IVigneshwar SNo ratings yet
- Open University of Tanzania Term PaperDocument7 pagesOpen University of Tanzania Term Paperafmzfmeeavndqe100% (1)
- Cultural Understanding Impacts Consumer BehaviorDocument10 pagesCultural Understanding Impacts Consumer BehaviorNguyễn Hữu Thảo NguyênNo ratings yet
- Ricoh Aficio SP c830dn-c831dn AP-p3 (m124-m125) FSMDocument1,064 pagesRicoh Aficio SP c830dn-c831dn AP-p3 (m124-m125) FSMDương Minh Phụng100% (1)
- Human Ear and Role of Hearing in HCIDocument4 pagesHuman Ear and Role of Hearing in HCIrafia0% (1)
- Cement and Concrete Research: Amin Abrishambaf, Mário Pimentel, Sandra NunesDocument13 pagesCement and Concrete Research: Amin Abrishambaf, Mário Pimentel, Sandra NunesJoseluis Dejesus AnguloNo ratings yet
- Imeko WC 2012 TC21 O10Document5 pagesImeko WC 2012 TC21 O10mcastillogzNo ratings yet
- 2narrative Essay - My Favorite TeacherDocument9 pages2narrative Essay - My Favorite TeacherHerbertKoh100% (1)
- Baxa Resumen PDFDocument12 pagesBaxa Resumen PDFChepe Camacho100% (3)
- Lean Healthy Raw Food Winter RecipesDocument60 pagesLean Healthy Raw Food Winter RecipesKaio Sol100% (6)
- National Capital Region Schools Division Office Novaliches High School MAPEH Department Definitive Budget of Work for Blended Learning Modality Quarter 1 Grade 10Document9 pagesNational Capital Region Schools Division Office Novaliches High School MAPEH Department Definitive Budget of Work for Blended Learning Modality Quarter 1 Grade 10Ma. Cristina Angenel RamosNo ratings yet
- TLC Visualization SolutionsDocument3 pagesTLC Visualization SolutionseraborNo ratings yet
- Khwaja Moinuddin Chishti Language UniversityDocument30 pagesKhwaja Moinuddin Chishti Language UniversityShivam ShuklaNo ratings yet
- Oromia State UniversityDocument65 pagesOromia State UniversityEYOB AHMEDNo ratings yet
- 255 Introduction Vocational Service enDocument12 pages255 Introduction Vocational Service enDmitri PopaNo ratings yet
- Weekly TestDocument12 pagesWeekly Testrossana rondaNo ratings yet
- Resilience WorkbookDocument54 pagesResilience WorkbookLeo Siu100% (1)
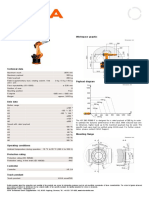
- KR 280 R3080 F technical specificationsDocument1 pageKR 280 R3080 F technical specificationsDorobantu CatalinNo ratings yet