You might also like
- 1 CombineDocument726 pages1 CombineSong Hành Vạn KiếpNo ratings yet
- VaccinesDocument4 pagesVaccinesSam smithNo ratings yet
- Adult Combined ScheduleDocument5 pagesAdult Combined SchedulelcmurilloNo ratings yet
- Philippine College of Chest Physicians: Media Kit For PneumoniaDocument4 pagesPhilippine College of Chest Physicians: Media Kit For PneumoniaWilsonne ChuaNo ratings yet
- Adult ScheduleDocument3 pagesAdult ScheduledrmanojvimalNo ratings yet
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Document4 pagesSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)gyna_2002No ratings yet
- Finally Vaccine (Uw + MTB) By: ArakiDocument4 pagesFinally Vaccine (Uw + MTB) By: Arakikoki74No ratings yet
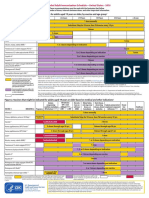
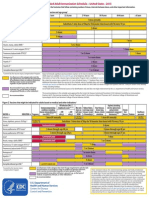
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocument2 pagesFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNo ratings yet
- Guidelines For Vaccination in Normal Adults in India - PMCDocument14 pagesGuidelines For Vaccination in Normal Adults in India - PMCSKMH INSURANCENo ratings yet
- Australian Technical Advisory Group On Immunisation (ATAGI)Document37 pagesAustralian Technical Advisory Group On Immunisation (ATAGI)Isa EnacheNo ratings yet
- Jama Sha 2019 It 190019Document2 pagesJama Sha 2019 It 190019xtineNo ratings yet
- Adult ScheduleDocument3 pagesAdult SchedulelcmurilloNo ratings yet
- Adult Immunization ScheduleDocument3 pagesAdult Immunization ScheduleBryan Mae H. DegorioNo ratings yet
- Adult Pocafeket SizeDocument2 pagesAdult Pocafeket SizedadfNo ratings yet
- Summary of Recommendations For Adult Immunization: (Age 19 Years and Older)Document5 pagesSummary of Recommendations For Adult Immunization: (Age 19 Years and Older)Hannah Caburian RemoNo ratings yet
- Pneumococcal Vaccination in AdultsDocument23 pagesPneumococcal Vaccination in AdultsIvelisse TaverasNo ratings yet
- Adult ImmunizationDocument6 pagesAdult ImmunizationAmit GoelNo ratings yet
- Varilrix SMPC JAN16Document10 pagesVarilrix SMPC JAN16TotochaNo ratings yet
- Hep B GuidelinesDocument8 pagesHep B GuidelinesHarold Von LeightonNo ratings yet
- Pneumococcal Conjugate: VaccineDocument2 pagesPneumococcal Conjugate: VaccineJenny TaylorNo ratings yet
- Vaccination in Special Situations SeminarDocument21 pagesVaccination in Special Situations SeminarDeep ShahNo ratings yet
- CDC Healthcare Personnel Vaccination RecommendationsDocument1 pageCDC Healthcare Personnel Vaccination RecommendationsdocktpNo ratings yet
- Current Presumptive Immunization SchedulesDocument4 pagesCurrent Presumptive Immunization SchedulesPedro Julian Tenorio ApesteguiNo ratings yet
- Greenbook Chapter 7 Immunsing ImmunosupressedDocument8 pagesGreenbook Chapter 7 Immunsing Immunosupressedحسام الدين إسماعيلNo ratings yet
- When Your Patient Has PneumoniaDocument4 pagesWhen Your Patient Has PneumoniaawuahbohNo ratings yet
- Antiviral Summary ClinicianDocument20 pagesAntiviral Summary ClinicianPurpleeyoreNo ratings yet
- Adult Immunization: It's Your Best Shot!Document40 pagesAdult Immunization: It's Your Best Shot!minerva_stanciuNo ratings yet
- AstraZeneca Vaccination Fact Sheet FINALDocument2 pagesAstraZeneca Vaccination Fact Sheet FINALAnaesthesia Intensive Care LecturerNo ratings yet
- Adult Schedule 11x17Document2 pagesAdult Schedule 11x17lcmurilloNo ratings yet
- Adult Combined ScheduleDocument6 pagesAdult Combined ScheduleAstrid Elaine RosalesNo ratings yet
- Splenectomy: DisclaimerDocument5 pagesSplenectomy: DisclaimerMimi FatinNo ratings yet
- Iap Guide Book On Immunization Immunization in Special Situations PDFDocument8 pagesIap Guide Book On Immunization Immunization in Special Situations PDFGirdhari Lal Saini100% (1)
- Adult ScheduleDocument3 pagesAdult ScheduleerilarchiNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument30 pagesDr. Ali's Uworld Notes For Step 2 CKuyesNo ratings yet
- Adult Combined ScheduleDocument5 pagesAdult Combined ScheduleAwal Safar MNo ratings yet
- COVID-19 Vaccine in Patients With Haematological Disorders British Society For HaematologyDocument10 pagesCOVID-19 Vaccine in Patients With Haematological Disorders British Society For HaematologydrToikNo ratings yet
- Guide To Contraindications and Precautions To Commonly Used VaccinesDocument2 pagesGuide To Contraindications and Precautions To Commonly Used VaccinesalbortoNo ratings yet
- Preventing and Treating Infections in Children With Asplenia or HypospleniaDocument5 pagesPreventing and Treating Infections in Children With Asplenia or HypospleniaAmélieNo ratings yet
- Stay Healthy, Stay On Top of Vaccinations: CDC Click Here For The CDC's Full Vaccination ChartDocument4 pagesStay Healthy, Stay On Top of Vaccinations: CDC Click Here For The CDC's Full Vaccination ChartcircularreasoningNo ratings yet
- Habits Are Some of The Strategies RecommendedDocument30 pagesHabits Are Some of The Strategies Recommendedmd.dascalescu2486No ratings yet
- Splenectomy - Factsheet - For - Health - Professionals 2022 FinalDocument4 pagesSplenectomy - Factsheet - For - Health - Professionals 2022 Finalalpha.blocker11No ratings yet
- Immunizations: Policies and Procedures: Intensive Care Nursery House Staff ManualDocument2 pagesImmunizations: Policies and Procedures: Intensive Care Nursery House Staff ManualSedaka DonaldsonNo ratings yet
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsRating: 5 out of 5 stars5/5 (9)
- Guide To Contraindications and Precautions To Commonly Used VaccinesDocument2 pagesGuide To Contraindications and Precautions To Commonly Used VaccinesMariana E. GutiérrezNo ratings yet
- Aufklaerungsbogen EnglischDocument20 pagesAufklaerungsbogen EnglischmillenialrefugeeNo ratings yet
- Immunization Routine Table1Document9 pagesImmunization Routine Table1MeeKo VideñaNo ratings yet
- Managing Immunosuppressant and Vaccination in Covid - Dr. Ravi SinghDocument26 pagesManaging Immunosuppressant and Vaccination in Covid - Dr. Ravi SinghJoel KennedyNo ratings yet
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Document4 pagesSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)enquzerNo ratings yet
- Swine Flu Swine Flu: Ministry of Health and Family Welfare Government of IndiaDocument19 pagesSwine Flu Swine Flu: Ministry of Health and Family Welfare Government of IndiagirismgNo ratings yet
- CPG On Immunization For WomenDocument28 pagesCPG On Immunization For WomenYnoli DiosomitoNo ratings yet
- Altered Immunocompetence: UpdatesDocument27 pagesAltered Immunocompetence: UpdatestrishnaNo ratings yet
- Typhoid Fever Follow-Up PDFDocument16 pagesTyphoid Fever Follow-Up PDFPlot BUnniesNo ratings yet
- Adult Combined Schedule VaccineDocument33 pagesAdult Combined Schedule VaccinehatsuneNo ratings yet
- Week 4 Peer ResponseDocument3 pagesWeek 4 Peer ResponseMayumi BalmesNo ratings yet
- Health Advice and Immunizations for TravelersFrom EverandHealth Advice and Immunizations for TravelersNo ratings yet
- ปริ้น Guideline-Vaccine-PneumoDocument5 pagesปริ้น Guideline-Vaccine-PneumoBoonyapart SorninNo ratings yet
- (MMUNISATIONDocument54 pages(MMUNISATIONatharva sawantNo ratings yet
- Table 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenDocument7 pagesTable 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenKrishnendu PramanikNo ratings yet
- Guide To Contraindications To VaccinationDocument2 pagesGuide To Contraindications To VaccinationGabriel GarrisonNo ratings yet
- Anaesthesia & Intensive Care: For Fcai, Frca EdaicDocument139 pagesAnaesthesia & Intensive Care: For Fcai, Frca EdaicMuhammad Farid100% (1)
- BLOOD - FinalDocument8 pagesBLOOD - FinalanuNo ratings yet
- Surfactant Final 2Document5 pagesSurfactant Final 2anuNo ratings yet
- Enteral Feeding of PretermDocument9 pagesEnteral Feeding of PretermanuNo ratings yet
- Echo OptimisationDocument86 pagesEcho OptimisationanuNo ratings yet
- MorphologyDocument52 pagesMorphologyanuNo ratings yet
- LPD Rev. 6 Pneumococcal 13-Valent Conjugate Vaccine - Prevenar 13 CLEANDocument34 pagesLPD Rev. 6 Pneumococcal 13-Valent Conjugate Vaccine - Prevenar 13 CLEANYana CovarNo ratings yet
- Final PresentationDocument43 pagesFinal Presentationapi-608681693No ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument30 pagesDr. Ali's Uworld Notes For Step 2 CKuyesNo ratings yet
- Pneumococcal Vaccine Timing For AdultsDocument4 pagesPneumococcal Vaccine Timing For AdultsNur Farhanah Zulkifli100% (1)
- France and Saudi ArabiaDocument17 pagesFrance and Saudi ArabiaHajar HossamNo ratings yet
- Imunisasi HajiDocument89 pagesImunisasi HajiFakikha AditamiNo ratings yet
- Name of Drug Classification Mechanism of Action Indication Contraindication Side Effects Nursing ResponsibilitiesDocument4 pagesName of Drug Classification Mechanism of Action Indication Contraindication Side Effects Nursing ResponsibilitiesMinaNo ratings yet
- Bioentrepreneur - Building A Life Science VentureDocument4 pagesBioentrepreneur - Building A Life Science VentureGenlajt DOOELNo ratings yet
- Look at Me Mommy!: Congratulations, Mommy and Daddy!Document26 pagesLook at Me Mommy!: Congratulations, Mommy and Daddy!Karen ValdezNo ratings yet
- Africa Health News May-June 2009Document4 pagesAfrica Health News May-June 2009simguybarNo ratings yet
- Vaccine Schedule Recommended Adults 2022 v03Document2 pagesVaccine Schedule Recommended Adults 2022 v03mariumNo ratings yet
- Published Immunogenicity and Safety of A Novel Ten-Valent PNDocument13 pagesPublished Immunogenicity and Safety of A Novel Ten-Valent PNIvan GeromeNo ratings yet
- Vaccines and Routine Immunization Strategies During The COVID 19 PandemicDocument9 pagesVaccines and Routine Immunization Strategies During The COVID 19 PandemicMěđ SimoNo ratings yet
- Data CTRI DataDocument5 pagesData CTRI DataDonvgmailNo ratings yet
- Ishimine2013fiebre SignosDocument26 pagesIshimine2013fiebre SignosAnirisulNo ratings yet
- Streptococcus Pneumoniae S. PneumoniaeDocument18 pagesStreptococcus Pneumoniae S. PneumoniaeadrianNo ratings yet
- 0-23 Monitoring FormDocument6 pages0-23 Monitoring FormKOBE TOMAGANNo ratings yet
- Pneumonia and Invasive Pneumococcal Diseases - The Role of Pneumococcal Conjugate Vaccine in The Era of Multi-Drug Resistance - PMCDocument33 pagesPneumonia and Invasive Pneumococcal Diseases - The Role of Pneumococcal Conjugate Vaccine in The Era of Multi-Drug Resistance - PMC90Agva Dwi FatikaNo ratings yet
- PRICE SURVEY - Vaccines Pricing Audit IndonesiaDocument10 pagesPRICE SURVEY - Vaccines Pricing Audit IndonesiaNur Farahiyah AmalinaNo ratings yet
- Test Bank For Introduction To Medical Surgical Nursing 4th Edition Adrianne D Linton Full DownloadDocument12 pagesTest Bank For Introduction To Medical Surgical Nursing 4th Edition Adrianne D Linton Full Downloadmelissapollardoxieprwsdb100% (40)
- 4th Regional Pneumococcal Symposium - DownloadableDocument64 pages4th Regional Pneumococcal Symposium - DownloadablesabinvaccineNo ratings yet
- Green Book Chapter 11Document9 pagesGreen Book Chapter 11VergaaBellanyNo ratings yet
- PH20-000531 SDV Pneumococcal 13-Valent Conjugate Vaccine Prevenar 13 VialDocument39 pagesPH20-000531 SDV Pneumococcal 13-Valent Conjugate Vaccine Prevenar 13 VialLoanne RamiterreNo ratings yet
- The Routine Immunisation Schedule: From Autumn 2018Document2 pagesThe Routine Immunisation Schedule: From Autumn 2018Adityo AriwibowoNo ratings yet
- Chapter 14-15, All Tables and Figures Taken From This ChapterDocument74 pagesChapter 14-15, All Tables and Figures Taken From This ChapterNour MohammedNo ratings yet
- Impact of Pneumococcal Conjugate Vaccine in At-Risk Adults 2022Document48 pagesImpact of Pneumococcal Conjugate Vaccine in At-Risk Adults 2022Rosi AmaliaNo ratings yet
- Vaccines, Cold Chain and Logistics Management: Manual of OperationsDocument148 pagesVaccines, Cold Chain and Logistics Management: Manual of Operationscesspintas Cuaresma67% (3)
- Immunizations Health TeachingDocument9 pagesImmunizations Health TeachingClaudine Jo B. TalabocNo ratings yet
- Immunisation ScheduleDocument3 pagesImmunisation SchedulejegathesmsjsNo ratings yet
- Convert I DoDocument43 pagesConvert I Do71403971No ratings yet