You might also like
- Blood Gas AnalysisDocument52 pagesBlood Gas AnalysisKresna Dharma SuryanaNo ratings yet
- Arterial Blood Gas Analysis - making it easyFrom EverandArterial Blood Gas Analysis - making it easyRating: 4.5 out of 5 stars4.5/5 (4)
- CCRN PulmonaryDocument107 pagesCCRN PulmonaryCzarina Charmaine Diwa100% (4)
- ABG Interpretation Guide: 4 Steps to Analyze Arterial Blood GasesDocument13 pagesABG Interpretation Guide: 4 Steps to Analyze Arterial Blood Gasesgwapz23No ratings yet
- Lung Function in Health and Disease Basic Concepts of Respiratory Physiology and PathophysiologyFrom EverandLung Function in Health and Disease Basic Concepts of Respiratory Physiology and PathophysiologyNo ratings yet
- USAF Mac Aikido New Student GuideDocument24 pagesUSAF Mac Aikido New Student GuideThumper KatesNo ratings yet
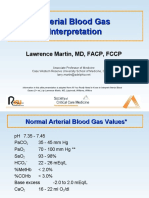
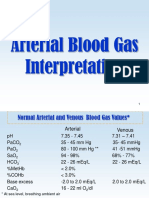
- Arterial Blood Gas InterpretationDocument65 pagesArterial Blood Gas InterpretationDaniel AryanNo ratings yet
- Arterial Blood GasDocument255 pagesArterial Blood GasMark Joshua S CruzNo ratings yet
- Acid Base ImbalanceDocument50 pagesAcid Base ImbalanceDian Pratiwi BurnamaNo ratings yet
- Kepler's Celestial MusicDocument24 pagesKepler's Celestial Musicfranciscoacfreitas100% (1)
- Credit Management Overview and Principles of LendingDocument44 pagesCredit Management Overview and Principles of LendingTavneet Singh100% (2)
- Gas ExchangeDocument15 pagesGas ExchangeOsolemio Mer100% (1)
- Abg Analysis ReviewerDocument21 pagesAbg Analysis ReviewerAyiessa_AJNo ratings yet
- Oet Reading Part A Additional - GlucomaDocument8 pagesOet Reading Part A Additional - Glucomaafacean25% (8)
- Stephen C. Wood, Ph.D. Medical Physiology Metabolic Rate and Alveolar VentilationDocument9 pagesStephen C. Wood, Ph.D. Medical Physiology Metabolic Rate and Alveolar VentilationSimran SukhijaNo ratings yet
- Ethics and Social ResponsibilityDocument16 pagesEthics and Social Responsibilitypallavi50% (2)
- Interpretation of Arterial Blood Gases and Acid-Base DisordersDocument44 pagesInterpretation of Arterial Blood Gases and Acid-Base DisordersSuren VishvanathNo ratings yet
- V/Q and Oxygen: Anuja Abayadeera Part 1B AnaesthsiologyDocument42 pagesV/Q and Oxygen: Anuja Abayadeera Part 1B Anaesthsiologyv_vijayakanth7656No ratings yet
- Stepwise approach to ABG interpretationDocument6 pagesStepwise approach to ABG interpretationYogeshRavalNo ratings yet
- Arterial Blood Gas Interpretation GuideDocument34 pagesArterial Blood Gas Interpretation GuideChristiana TrijayantiNo ratings yet
- Arterial Blood Gas AnalysisDocument23 pagesArterial Blood Gas AnalysisVartika SainiNo ratings yet
- Arterial Blood Gas: Interpretation and Clinical ImplicationsDocument112 pagesArterial Blood Gas: Interpretation and Clinical ImplicationsmatrixtrinityNo ratings yet
- AbgDocument66 pagesAbgIan OrwaNo ratings yet
- ABGDocument16 pagesABGKesavanVeeraNo ratings yet
- Abg AnalysisDocument65 pagesAbg AnalysisSyed Farooque AliNo ratings yet
- Y5 RN - Abgs 27oct2010Document5 pagesY5 RN - Abgs 27oct2010Canh VanNo ratings yet
- ABG QuizDocument13 pagesABG QuizSSNo ratings yet
- Oxygen Therapy: Dr. Rajesh AroraDocument59 pagesOxygen Therapy: Dr. Rajesh ArorarkdivyaNo ratings yet
- Arterial Blood Gas InterpretationDocument66 pagesArterial Blood Gas InterpretationkabatchinoooNo ratings yet
- ABG Made EasyDocument9 pagesABG Made EasyDrShruthi PradeepNo ratings yet
- Arterial Blood Gas InterpretationDocument66 pagesArterial Blood Gas InterpretationlenafitriyaniNo ratings yet
- Causes of Low Oxygen in Blood (HypoxemiaDocument6 pagesCauses of Low Oxygen in Blood (HypoxemiaSamantha LuiNo ratings yet
- ABG QuizDocument12 pagesABG QuizParsaant SinghNo ratings yet
- Blood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical CareDocument48 pagesBlood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical Carehagir alhajNo ratings yet
- Arterial Blood Gas InterpretationDocument69 pagesArterial Blood Gas InterpretationostuffeNo ratings yet
- Interpreting Blood Gases Easy As Abc PDFDocument6 pagesInterpreting Blood Gases Easy As Abc PDFmuhammad hidayahNo ratings yet
- Arterial Blood Gas.Document4 pagesArterial Blood Gas.Sathish KumarNo ratings yet
- Blood Gas AnalysisDocument5 pagesBlood Gas Analysissraji64No ratings yet
- Blood Gas Analysis: Respiratory DisordersDocument15 pagesBlood Gas Analysis: Respiratory DisordersYogeshRavalNo ratings yet
- Oxygen Cascade - SHANTHINIDocument57 pagesOxygen Cascade - SHANTHINIMani BharathiNo ratings yet
- Rules and Equations for Oxygen Therapy and Gas ExchangeDocument11 pagesRules and Equations for Oxygen Therapy and Gas ExchangeJenn77x1No ratings yet
- Analisis Gas DarahDocument2 pagesAnalisis Gas DarahTri GunawanNo ratings yet
- Analisis Gas DarahDocument2 pagesAnalisis Gas DarahTri GunawanNo ratings yet
- Arterial Blood Gas Workshop Dr. Lanzona 12.06.07: Lala 3C-Med-09 1Document4 pagesArterial Blood Gas Workshop Dr. Lanzona 12.06.07: Lala 3C-Med-09 1pramastutiNo ratings yet
- ABG Interpretation: Normal Ranges 2. PHDocument2 pagesABG Interpretation: Normal Ranges 2. PHAlexander EnnesNo ratings yet
- AbgDocument48 pagesAbgzhaimeangirlNo ratings yet
- Abg InterpretationDocument52 pagesAbg InterpretationCirugia Cardiovascular NeivaNo ratings yet
- Hypoxia: Moderator: DR Meera Balasubramanyam Professor Dept of Anaesthesiology MMCRI Speaker: DR Nandhini.K.S.KaratDocument65 pagesHypoxia: Moderator: DR Meera Balasubramanyam Professor Dept of Anaesthesiology MMCRI Speaker: DR Nandhini.K.S.KaratAnn Susan MathewNo ratings yet
- ABG GeekymedicsDocument13 pagesABG Geekymedicscharlyn206No ratings yet
- Acid BaseDocument6 pagesAcid BaseCarol Solanyi Gacha QuinteroNo ratings yet
- AbgDocument66 pagesAbgindyaphdNo ratings yet
- Respiratory Physiology Airway Resistance and Pulmonary Function TestingDocument41 pagesRespiratory Physiology Airway Resistance and Pulmonary Function TestingEdwin OkonNo ratings yet
- LRP CriticalCare Sample2Document46 pagesLRP CriticalCare Sample2Aniket ChoudharyNo ratings yet
- Review of Respiratory PhysiologyDocument46 pagesReview of Respiratory Physiologylovelyc95No ratings yet
- 4) Physiology-Acid Base Balance-PFTsDocument43 pages4) Physiology-Acid Base Balance-PFTsbikedet268No ratings yet
- O2 Transpot & DeliveryDocument42 pagesO2 Transpot & Deliverypprashant00100% (2)
- O2 Therapy, ABGs & InterpretationDocument4 pagesO2 Therapy, ABGs & InterpretationPebblesNo ratings yet
- ABG5oct2010 FinalDocument54 pagesABG5oct2010 FinalAmit Kocheta100% (1)
- Oxygen Concentration of Blood: Key Concepts and MeasurementsDocument33 pagesOxygen Concentration of Blood: Key Concepts and MeasurementskareemNo ratings yet
- ABG InterpretationDocument13 pagesABG InterpretationAbid KhanNo ratings yet
- Causes of Hypoxemia: VA/Q Inequality Most CommonDocument6 pagesCauses of Hypoxemia: VA/Q Inequality Most CommonZoherNBezantiNo ratings yet
- Arterial Blood GasDocument33 pagesArterial Blood GaskartikaparamitaNo ratings yet
- Abnormal Ventilation, Abnormal Gas ExchangeDocument52 pagesAbnormal Ventilation, Abnormal Gas ExchangekateNo ratings yet
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- PETDocument21 pagesPETmahmod omerNo ratings yet
- HRCT Findings of Lung Disease ClassificationDocument82 pagesHRCT Findings of Lung Disease Classificationmahmod omerNo ratings yet
- Oxygen TherapyDocument83 pagesOxygen Therapymahmod omerNo ratings yet
- Niv in CopdDocument54 pagesNiv in Copdmahmod omerNo ratings yet
- F18 - FDG PetDocument18 pagesF18 - FDG Petmahmod omerNo ratings yet
- LVRSDocument52 pagesLVRSmahmod omerNo ratings yet
- Solitary Pulmonary Nodule (SPN (Document59 pagesSolitary Pulmonary Nodule (SPN (mahmod omerNo ratings yet
- ImunotherapyDocument57 pagesImunotherapymahmod omerNo ratings yet
- Abx in CopdDocument34 pagesAbx in Copdmahmod omerNo ratings yet
- Aisha Isyaku Term PaperDocument27 pagesAisha Isyaku Term PaperUsman Ahmad TijjaniNo ratings yet
- Purposive Communication - WK 3Document7 pagesPurposive Communication - WK 3Alexandre QuintoNo ratings yet
- The Seven C's of Effective Business CommunicationDocument102 pagesThe Seven C's of Effective Business CommunicationKainat BaigNo ratings yet
- Cainta Catholic College: Senior High School DepartmentDocument17 pagesCainta Catholic College: Senior High School DepartmentAllan Santos SalazarNo ratings yet
- Google App Engine: A Platform for Developing and Hosting Web AppsDocument5 pagesGoogle App Engine: A Platform for Developing and Hosting Web AppsnagrajNo ratings yet
- Concrete Creep PropertiesDocument49 pagesConcrete Creep PropertiesGurram VinayNo ratings yet
- Cardiology OSCEDocument35 pagesCardiology OSCEvigneshmmc02No ratings yet
- Four Theories of the Press - Libertarian vs AuthoritarianDocument8 pagesFour Theories of the Press - Libertarian vs Authoritarianআলটাফ হুছেইনNo ratings yet
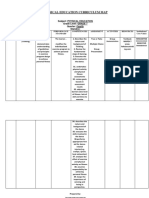
- Physical Education Curriculum MapDocument20 pagesPhysical Education Curriculum MapdyonaraNo ratings yet
- Practice Grammar Part2Document4 pagesPractice Grammar Part2Lightning StrifeNo ratings yet
- Domestic Violence Cycle of Violence Types of Families-2Document22 pagesDomestic Violence Cycle of Violence Types of Families-2api-340420872No ratings yet
- Principles and Stategies in Teaching MathDocument35 pagesPrinciples and Stategies in Teaching MathGeraldine RamosNo ratings yet
- Actron CP9449 User ManualDocument58 pagesActron CP9449 User ManualMichael BongioviNo ratings yet
- Tom PN 101215Document62 pagesTom PN 101215JustinTangNo ratings yet
- Phrasal Verbs2 - Revisión Del Intento2Document4 pagesPhrasal Verbs2 - Revisión Del Intento2Rocio A RubecindoNo ratings yet
- AsianJPharmHealthSci 2-3-428Document5 pagesAsianJPharmHealthSci 2-3-428KkanuPriyaNo ratings yet
- SEAL MIDTERM - EditedDocument6 pagesSEAL MIDTERM - EditedJames SajolNo ratings yet
- Nmat Test Result-1017051213Document1 pageNmat Test Result-1017051213Dushyant SarvaiyaNo ratings yet
- Leading culturally diverse global teamsDocument20 pagesLeading culturally diverse global teamsEdrick SoegiantoNo ratings yet
- Gestalt Principles 1Document56 pagesGestalt Principles 1Moiz AhmadNo ratings yet
- Lo Visual en YourcenarDocument272 pagesLo Visual en YourcenarJosé Ignacio Herrera LamasNo ratings yet
- History of Anglo Saxon Literature English Assignment NUML National University of Modern LanguagesDocument15 pagesHistory of Anglo Saxon Literature English Assignment NUML National University of Modern LanguagesMaanNo ratings yet
- 9601 Be Quiet George The ImperativeDocument1 page9601 Be Quiet George The Imperativeheoquay19311% (9)
- BadjaoDocument3 pagesBadjaochristianpauloNo ratings yet