You might also like
- Co-signal Molecules in T Cell Activation: Immune Regulation in Health and DiseaseFrom EverandCo-signal Molecules in T Cell Activation: Immune Regulation in Health and DiseaseMiyuki AzumaNo ratings yet
- Non-inflammatory immunology: An introduction to the immune system and its pathologiesFrom EverandNon-inflammatory immunology: An introduction to the immune system and its pathologiesNo ratings yet
- Asthma Pathophysiology TheraDocument3 pagesAsthma Pathophysiology TheraJayde TabanaoNo ratings yet
- 4.chronic InflammationDocument29 pages4.chronic Inflammationyaqeenallawi23No ratings yet
- Cytokines: An Overview of Their Classification, Functions and Role in Rheumatoid ArthritisDocument39 pagesCytokines: An Overview of Their Classification, Functions and Role in Rheumatoid ArthritisRiska Resty WasitaNo ratings yet
- Unit 6 CytokinesDocument29 pagesUnit 6 CytokinesamirahaliNo ratings yet
- Cytokine Roles and Functions in the Immune SystemDocument53 pagesCytokine Roles and Functions in the Immune SystemBima Ewando KabanNo ratings yet
- Cytokines & Their ActionsDocument59 pagesCytokines & Their ActionsSharanabasappa DurgNo ratings yet
- Asthma - PROF WASEEM (2022)Document36 pagesAsthma - PROF WASEEM (2022)Mahnoor AyeshaNo ratings yet
- Cytokines N ChemokionesDocument31 pagesCytokines N ChemokionesMd. Ahsan-Ul BariNo ratings yet
- Cytokine Functions and Receptor FamiliesDocument6 pagesCytokine Functions and Receptor FamiliesNur LiyanaNo ratings yet
- Immunologic Mechanisms in AsthmaDocument9 pagesImmunologic Mechanisms in AsthmaKessi VikaneswariNo ratings yet
- Helper T Cells and CytokinesDocument3 pagesHelper T Cells and CytokinesSubashan VadibelerNo ratings yet
- Cytokines: General Properties and Role in Innate and Adaptive ImmunityDocument50 pagesCytokines: General Properties and Role in Innate and Adaptive ImmunityKhalil KhusairiNo ratings yet
- Activation of T Lymphocytes: Hypersensitivity Referring To Tissue Damage Caused by An ImmuneDocument8 pagesActivation of T Lymphocytes: Hypersensitivity Referring To Tissue Damage Caused by An ImmuneJorge SalinasNo ratings yet
- Innate Immunity 3 (50 Q)Document5 pagesInnate Immunity 3 (50 Q)evelynseaaNo ratings yet
- CytokinesDocument3 pagesCytokinesMohanad JawadNo ratings yet
- CytokineDocument7 pagesCytokineMaryam ShahrasbiNo ratings yet
- HBB 2306 Notes IIDocument14 pagesHBB 2306 Notes IIfelixNo ratings yet
- TNF Superfamily and ILC2 Activation in Asthma by Takahiro Matsuyama, Brittany Marie Salter, Nahal Emami Fard, Kentaro Machida Androma SehmiDocument19 pagesTNF Superfamily and ILC2 Activation in Asthma by Takahiro Matsuyama, Brittany Marie Salter, Nahal Emami Fard, Kentaro Machida Androma SehmiTedNo ratings yet
- Topic: Cytokine and Their Roles in The Immune Regulation: Md. Jiyaul MustafaDocument21 pagesTopic: Cytokine and Their Roles in The Immune Regulation: Md. Jiyaul MustafaAisha Siddiq100% (1)
- Cell-Mediated ImmunityDocument15 pagesCell-Mediated ImmunityFatema Al-KananiNo ratings yet
- Advances in treating allergic diseases and asthma through immunological approachesDocument17 pagesAdvances in treating allergic diseases and asthma through immunological approachesSam SonNo ratings yet
- Aktivasi Sel TDocument3 pagesAktivasi Sel TVictoria DeathenNo ratings yet
- Up To Date. Pathogenesis of Allergic RhinitisDocument16 pagesUp To Date. Pathogenesis of Allergic RhinitisGuardito PequeñoNo ratings yet
- Immunity Innate Immunity: When The Going Gets Tough, The Tough Gets Going...Document7 pagesImmunity Innate Immunity: When The Going Gets Tough, The Tough Gets Going...dtimtimanNo ratings yet
- AsthmaDocument100 pagesAsthmaMohamed HefnyNo ratings yet
- Tugas Imunologi Dasar Fast TrackDocument23 pagesTugas Imunologi Dasar Fast TrackAnditri WeningtyasNo ratings yet
- Cytokines 1Document18 pagesCytokines 1Heba AlNo ratings yet
- Clinical Flow Cytometry - Emerging ApplicationsDocument215 pagesClinical Flow Cytometry - Emerging ApplicationsDaoud IssaNo ratings yet
- ABBAS BAB 2 Innate ImmunityDocument28 pagesABBAS BAB 2 Innate ImmunitydianaNo ratings yet
- Study Guide: Cytokines Associated With Innate ImmunityDocument12 pagesStudy Guide: Cytokines Associated With Innate ImmunityxxxxxxxNo ratings yet
- Lymphokines & Cytokines: Immunology & DiseaseDocument34 pagesLymphokines & Cytokines: Immunology & DiseasejaneNo ratings yet
- Cells and Mediators of Chronic InflammationDocument4 pagesCells and Mediators of Chronic InflammationRaquel Spiegel VieiraNo ratings yet
- Pathophysiology: RoductionDocument6 pagesPathophysiology: RoductionDhila SafirinaNo ratings yet
- Innate and Adaptive Immunity: - Innate Is FIRST LINE OF DEFENCE: No Prior Exposure Needed - Comprised OfDocument31 pagesInnate and Adaptive Immunity: - Innate Is FIRST LINE OF DEFENCE: No Prior Exposure Needed - Comprised OfBegumHazinNo ratings yet
- Ishaque PK Pondicherry UniversityDocument34 pagesIshaque PK Pondicherry UniversityRiska Resty WasitaNo ratings yet
- Slide Jurnal 1Document19 pagesSlide Jurnal 1Benni Andica SuryaNo ratings yet
- Basic Immunology of Allergic Disease: Tutik Ida Rosanti Laboratorium ParasitologiDocument17 pagesBasic Immunology of Allergic Disease: Tutik Ida Rosanti Laboratorium ParasitologiFiqrotul UmamNo ratings yet
- SGD 23 - Immunology 3Document4 pagesSGD 23 - Immunology 3John RayNo ratings yet
- MastCell-fibrosis - Rev 2018Document8 pagesMastCell-fibrosis - Rev 2018Banchob SripaNo ratings yet
- Cytokines in The Innate Immune ResponseDocument3 pagesCytokines in The Innate Immune ResponseNicole Tan100% (1)
- Essay ImmuneDocument8 pagesEssay ImmuneAishah Najihah100% (1)
- InflammationDocument28 pagesInflammationMasum ShahriarNo ratings yet
- Chapter 11:: Cytokines:: Ifor R. Williams & Thomas S. KupperDocument26 pagesChapter 11:: Cytokines:: Ifor R. Williams & Thomas S. KupperSartika Ayu NingsihNo ratings yet
- Chapter07 CytokinesDocument36 pagesChapter07 CytokinesLogical SolutionsNo ratings yet
- Perspectives: Diversification of T-Helper-Cell Lineages: Finding The Family Root of IL-17-producing CellsDocument5 pagesPerspectives: Diversification of T-Helper-Cell Lineages: Finding The Family Root of IL-17-producing CellsIván DiazNo ratings yet
- Ishaque PK Pondicherry UniversityDocument34 pagesIshaque PK Pondicherry UniversityharishchaudhariNo ratings yet
- Immunology (Session 13) ch13 Induction Cellular ResponseDocument12 pagesImmunology (Session 13) ch13 Induction Cellular ResponseHassan SleimanNo ratings yet
- Session 10 Chronic InflammationDocument40 pagesSession 10 Chronic InflammationGodfrey GeorgeNo ratings yet
- SITOKINDocument16 pagesSITOKINRidwan OorNo ratings yet
- 12-Cytokines 2020-2Document26 pages12-Cytokines 2020-2Rami AlhilliNo ratings yet
- CytokinesDocument36 pagesCytokinesAbdul KabirNo ratings yet
- Patomekanisme Bercak MerahDocument4 pagesPatomekanisme Bercak MerahsriNo ratings yet
- Principles of innate immunity (Abbas Chapter 4Document31 pagesPrinciples of innate immunity (Abbas Chapter 4foreveraldyNo ratings yet
- 1 Melatonin Prevents Allergic Airway Inflammation in Epicutaneously Sensitized MiceDocument12 pages1 Melatonin Prevents Allergic Airway Inflammation in Epicutaneously Sensitized Micebemfisio.cristianeribeiroNo ratings yet
- Chemical Mediators of Acute Inflammation - HandoutDocument24 pagesChemical Mediators of Acute Inflammation - HandoutRawa MuhsinNo ratings yet
- Immuno BiologyDocument111 pagesImmuno BiologyAsyha KantifaNo ratings yet
- Differentiation of Cd8+ T Cells Into Effector Ctls InvolvesDocument6 pagesDifferentiation of Cd8+ T Cells Into Effector Ctls InvolvesMutaz KhatatbehNo ratings yet
- Current Understanding of Asthma Pathogenesis and BiomarkersDocument17 pagesCurrent Understanding of Asthma Pathogenesis and BiomarkersRodríguez PabloNo ratings yet
- Live deer placenta stem cells not found in food supplement capsulesDocument1 pageLive deer placenta stem cells not found in food supplement capsulesJohn LêNo ratings yet
- BlsDocument62 pagesBlspaediatrica89% (19)
- Grizz Phys Tier 2 PDFDocument19 pagesGrizz Phys Tier 2 PDFJ VivianNo ratings yet
- Lifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsDocument7 pagesLifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsArcelino Farias100% (1)
- Connectors 2Document14 pagesConnectors 2Irene SánchezNo ratings yet
- Careers Surrey 20181Document15 pagesCareers Surrey 20181Kevin_Nguyen117No ratings yet
- Press Final - Abstract Book PDFDocument157 pagesPress Final - Abstract Book PDFAmbesh JhaNo ratings yet
- Que No4 & 5-With Clues and Without CluesDocument4 pagesQue No4 & 5-With Clues and Without CluesMir Yamin Uddin ZidanNo ratings yet
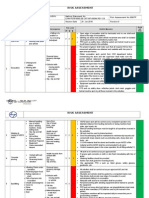
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- Assist LetterDocument2 pagesAssist Lettertashy richardsNo ratings yet
- 8 RA 4688 (Clinical Laboratory Law)Document32 pages8 RA 4688 (Clinical Laboratory Law)AIRRA CLAIRE ALVAREZNo ratings yet
- Melidiosis FDocument24 pagesMelidiosis FVyramuthu AtputhanNo ratings yet
- CYBERBULLYINGDocument2 pagesCYBERBULLYINGAdinda CahayaNo ratings yet
- 9 Types of Female Orgasms ExplainedDocument4 pages9 Types of Female Orgasms ExplainedAbdul SyukurNo ratings yet
- CPT 2021 guide for identifying medical proceduresDocument7 pagesCPT 2021 guide for identifying medical proceduresChester FernandezNo ratings yet
- Ent Solved Kmu Seqs by RMC StudentsDocument68 pagesEnt Solved Kmu Seqs by RMC StudentsAamir Khan100% (1)
- Obamacare Ushers in New Era For The Healthcare IndustryDocument20 pagesObamacare Ushers in New Era For The Healthcare Industryvedran1980No ratings yet
- Risk For Infection Related To Presence of Surgical Wounds As Evidenced by MER 2nd DegreeDocument3 pagesRisk For Infection Related To Presence of Surgical Wounds As Evidenced by MER 2nd DegreeSenyorita KHaye75% (12)
- Borderline Personality DisorderDocument7 pagesBorderline Personality DisorderleaNo ratings yet
- POne MPFFL 7 RV VPSX LQRPDocument3 pagesPOne MPFFL 7 RV VPSX LQRPRavi KumarNo ratings yet
- KPJ Pasir Gudang Covid Test ReportDocument1 pageKPJ Pasir Gudang Covid Test ReportNooh DinNo ratings yet
- Unit 1-Omd553-Telehealth TechnologyDocument53 pagesUnit 1-Omd553-Telehealth TechnologyjgjeslinNo ratings yet
- Should Homework Be Banned From School?Document7 pagesShould Homework Be Banned From School?Chuyên ĐỗNo ratings yet
- 4) Skema Set 1Document10 pages4) Skema Set 1Raymond Cheang Chee-CheongNo ratings yet
- Media Kesehatan Masyarakat: Gracewati Rambu Ladu Day, Muntasir Basri, Rina Waty SiraitDocument15 pagesMedia Kesehatan Masyarakat: Gracewati Rambu Ladu Day, Muntasir Basri, Rina Waty Siraitnimas ayu kusumaningrumNo ratings yet
- Change Your Life in 7 Days With NLP - Paul Mckenna BrochureDocument2 pagesChange Your Life in 7 Days With NLP - Paul Mckenna Brochureapi-385316675% (4)
- Ultrasound-Guided Lumbar Central Neuraxial Block 2016Document8 pagesUltrasound-Guided Lumbar Central Neuraxial Block 2016drkis20100% (1)
- Hazards of Nitrogen AsphyxiationDocument10 pagesHazards of Nitrogen AsphyxiationRaja Senthil NathanNo ratings yet
- Prevalence of GERD in Dyspepsia PatientsDocument6 pagesPrevalence of GERD in Dyspepsia PatientsAbrar TaraNo ratings yet
- ResistanceDocument8 pagesResistanceAndi Soraya WalyddainiNo ratings yet