You might also like
- Tubercular MeningitisDocument60 pagesTubercular MeningitisVRUSHAB PARAPPANAVARNo ratings yet
- Module 3. E-BookDocument16 pagesModule 3. E-Bookkaren solibaNo ratings yet
- Smear Negative TBDocument53 pagesSmear Negative TBsyuhaida deqsuNo ratings yet
- A View On TB ControlDocument30 pagesA View On TB ControlhonorinanuguidNo ratings yet
- Acierto, Dyvi Karen T. Catanyag, Hussein E. Ignacio, Karen G. Palanca, AriesDocument32 pagesAcierto, Dyvi Karen T. Catanyag, Hussein E. Ignacio, Karen G. Palanca, AriesBea MagnoNo ratings yet
- IAP consensus on diagnosing and treating childhood tuberculosisDocument15 pagesIAP consensus on diagnosing and treating childhood tuberculosisTammy Utami DewiNo ratings yet
- TB PDFDocument92 pagesTB PDFPrincess Cate MercadoNo ratings yet
- Diagnosis and Treatment of TB Under RNTCPDocument105 pagesDiagnosis and Treatment of TB Under RNTCPGunjan UpadhyayNo ratings yet
- Pediatric Tuberculosis: Specimen Collection For Analysis Sputum Specimens - Used in OlderDocument3 pagesPediatric Tuberculosis: Specimen Collection For Analysis Sputum Specimens - Used in OldernadiahNo ratings yet
- 2013 - To Xray or Not To Xray Screening Asymptomatic Children For Pulmonary TB A Retrospective AuditDocument5 pages2013 - To Xray or Not To Xray Screening Asymptomatic Children For Pulmonary TB A Retrospective AuditTammy Utami DewiNo ratings yet
- TB Screening and Diagnosis GuideDocument18 pagesTB Screening and Diagnosis GuideGloriana Julia TeopeNo ratings yet
- Tuberculosis PowerpointDocument69 pagesTuberculosis PowerpointCeline Villo100% (1)
- PK - Aspek Laboratorium Respirasi - Dr. AnnaDocument48 pagesPK - Aspek Laboratorium Respirasi - Dr. AnnaMUHAMMAD ILHAM PRATAMANo ratings yet
- TB Skin Test ExplainedDocument5 pagesTB Skin Test ExplainedRenrenz PayumoNo ratings yet
- Pediatric TB Diagnosis UpdatesDocument39 pagesPediatric TB Diagnosis UpdatesSiddhartha NandiNo ratings yet
- TB Idots Referring FacilityDocument18 pagesTB Idots Referring FacilityMikhaelEarlSantosTacorda100% (1)
- Pedia Pulmo 3Document48 pagesPedia Pulmo 3Sven OrdanzaNo ratings yet
- IGRA / Tuberculin Skin Test: DR - Haifa NaserDocument32 pagesIGRA / Tuberculin Skin Test: DR - Haifa NaserChristoper PratamaNo ratings yet
- National TB Control ProgramDocument45 pagesNational TB Control ProgramKim Michael PabatangNo ratings yet
- Homberg H 2009Document7 pagesHomberg H 2009abbhyasa5206No ratings yet
- Q&A Oslo Revisi 61023Document10 pagesQ&A Oslo Revisi 61023syukriNo ratings yet
- Mycobacteria BPTDocument26 pagesMycobacteria BPTbpt2No ratings yet
- Microbial Diagnostic NTMDocument12 pagesMicrobial Diagnostic NTMdicky wahyudiNo ratings yet
- Daftar Pustaka No 6Document11 pagesDaftar Pustaka No 6Efti WeaslyNo ratings yet
- Communicable Disease Nursing Part II DiseasesDocument21 pagesCommunicable Disease Nursing Part II DiseasesMicah EllaNo ratings yet
- Pulmonary Tuberculosis in ChildrenDocument26 pagesPulmonary Tuberculosis in ChildrenFAMED RESIDENTS CESMEDNo ratings yet
- TB CPG SummaryDocument14 pagesTB CPG SummaryErrold Joseph LahaganNo ratings yet
- PERTUSISDocument28 pagesPERTUSISFaridNorNo ratings yet
- A New Algorithm To Diagnose Tuberculosis in Children in IndonesiaDocument29 pagesA New Algorithm To Diagnose Tuberculosis in Children in IndonesiaRifny Hanifah SyawalNo ratings yet
- TB Management 2020 IPDocument5 pagesTB Management 2020 IPMohammed EliasNo ratings yet
- Mycobacterium Tuberculosis ThesisDocument5 pagesMycobacterium Tuberculosis Thesisamandagraytulsa100% (2)
- Differentiating Between CAP and TuberculosisDocument36 pagesDifferentiating Between CAP and TuberculosisMd Azhar InamdarNo ratings yet
- TB Symptoms Diagnosis TreatmentDocument2 pagesTB Symptoms Diagnosis Treatmentjust-maybe202No ratings yet
- Tuberclosis 1111Document33 pagesTuberclosis 1111elona jcimlNo ratings yet
- Comparison of Serum Neopterin Levels in Pulmonary Tuberculosis PatientsDocument3 pagesComparison of Serum Neopterin Levels in Pulmonary Tuberculosis PatientsParluhutan DolliNo ratings yet
- Mse) !) P (8x9e. h4, DDocument15 pagesMse) !) P (8x9e. h4, DKristel AnneNo ratings yet
- 89 12 08 Bazamozi Markaz Behdasht Diagnosis of TBDocument45 pages89 12 08 Bazamozi Markaz Behdasht Diagnosis of TBvijaya_vijju_1586982No ratings yet
- Ikm TBDocument72 pagesIkm TBAlfina Aulia RizkiNo ratings yet
- Pathology of TuberculosisDocument51 pagesPathology of TuberculosisChristopher YoungNo ratings yet
- 3 - Screening For Tuberculosis v02142020Document23 pages3 - Screening For Tuberculosis v02142020RHU MinalabacNo ratings yet
- Tuberculosis: Clinical Clerk Tanya Marie P. FernandezDocument72 pagesTuberculosis: Clinical Clerk Tanya Marie P. Fernandezbekbekk cabahugNo ratings yet
- 6 COMMUNICABLE DISEASES Nies PDocument14 pages6 COMMUNICABLE DISEASES Nies PMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- Tuberculosis UNIVALLEDocument33 pagesTuberculosis UNIVALLEPaz VidaNo ratings yet
- Approach To Child With Fever: Liew Qian YiDocument33 pagesApproach To Child With Fever: Liew Qian YinavenNo ratings yet
- Progressive Primary Tuberculosis in a 15-Month Old Male InfantDocument1 pageProgressive Primary Tuberculosis in a 15-Month Old Male InfantRenierose AgujetasNo ratings yet
- Tuberculosis 022007 HartDocument68 pagesTuberculosis 022007 HartWildan HumairahNo ratings yet
- Tuberculosis: Group #2 MembersDocument31 pagesTuberculosis: Group #2 MembersAudrey DelfinNo ratings yet
- Pengenalan TB, Diagnosis, Dan Pengobatannya FKM 2019Document47 pagesPengenalan TB, Diagnosis, Dan Pengobatannya FKM 2019yuly rahmawatiNo ratings yet
- Pediatri Essensial 3Document91 pagesPediatri Essensial 3alfred tristian giamNo ratings yet
- Fever With A Focus in Well Looking Child Under 3 YrsDocument80 pagesFever With A Focus in Well Looking Child Under 3 YrsAnuradha RoopchandNo ratings yet
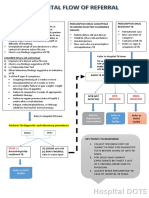
- Hospital DOTS: Identify PRESUMPTIVE TB CaseDocument1 pageHospital DOTS: Identify PRESUMPTIVE TB CaseYram Yoj ZeraujNo ratings yet
- Pediatri Essensial 3Document86 pagesPediatri Essensial 3Gregorius WahyudiNo ratings yet
- Diagnosis TBDocument44 pagesDiagnosis TBGede Eka Putra NugrahaNo ratings yet
- CSS TuberkulosisDocument69 pagesCSS TuberkulosisdhaniNo ratings yet
- Neonatal Sepsis Diagnosis and TreatmentDocument46 pagesNeonatal Sepsis Diagnosis and Treatment'-dooublleaiienn Itouehh IinNo ratings yet
- Pediatri Essensial Koas 3Document91 pagesPediatri Essensial Koas 3dewi novitasariNo ratings yet
- Tuberculosis or TBDocument8 pagesTuberculosis or TBJ Russel DichosoNo ratings yet
- Prolonged Sputum AFB 1-24-12Document10 pagesProlonged Sputum AFB 1-24-12Frits van der Kuyp, MD, MPH,FCCPNo ratings yet
- Improving household hygiene through nursing evaluation and interventionDocument1 pageImproving household hygiene through nursing evaluation and interventionCarmel VenezuelaNo ratings yet
- Jibrail Jilalu Thesis Final CommentDocument30 pagesJibrail Jilalu Thesis Final CommentJilalu SemanNo ratings yet
- Complete Hospital Discharge FormDocument2 pagesComplete Hospital Discharge Formepi bahoNo ratings yet
- Castro Domestic PoliciesDocument6 pagesCastro Domestic PoliciesAriana ChaconNo ratings yet
- Mental Health Coaching in the Church (39Document7 pagesMental Health Coaching in the Church (39Dr. Janeide A Matthews ChillisNo ratings yet
- Nepafenac An Ophthalmic Nonsteroidal Antiinflammatory DrugDocument6 pagesNepafenac An Ophthalmic Nonsteroidal Antiinflammatory DrugLalo ZaraloNo ratings yet
- BPSU Nursing Case Study: Labor and DeliveryDocument3 pagesBPSU Nursing Case Study: Labor and DeliveryMarielle CatainaNo ratings yet
- Health10 Q1 L1Document12 pagesHealth10 Q1 L1Jan Den Saul DalanNo ratings yet
- Midwifery Board Exam November 2014 Performance of SchoolsDocument11 pagesMidwifery Board Exam November 2014 Performance of SchoolsPRC BoardNo ratings yet
- SepsisDocument10 pagesSepsisJessa MaeNo ratings yet
- Efficacy For Treatment Anxiety DisordersDocument10 pagesEfficacy For Treatment Anxiety DisordersAnderson GaldinoNo ratings yet
- Icd X Dan Icd 9 CM Who Dentistry: International Statistical Classification of Diseases and Related Health ProblemsDocument25 pagesIcd X Dan Icd 9 CM Who Dentistry: International Statistical Classification of Diseases and Related Health ProblemsElon LiliNo ratings yet
- Park, 2019 - NEJM - DepressionDocument10 pagesPark, 2019 - NEJM - DepressionFabian WelchNo ratings yet
- Andhika Pangestu CVDocument6 pagesAndhika Pangestu CVPangestu DhikaNo ratings yet
- Getinge Hs33 Hospital SterilizerDocument8 pagesGetinge Hs33 Hospital SterilizerGhozy AnamNo ratings yet
- Bài tập của Trí 19032022Document6 pagesBài tập của Trí 19032022Minh TríNo ratings yet
- GEMP 4 EBM Assignment Template 2020Document9 pagesGEMP 4 EBM Assignment Template 2020Chanel Van Der WesthuizenNo ratings yet
- PN Nursing+care+plan+template (1) wk2Document3 pagesPN Nursing+care+plan+template (1) wk2api-282321350No ratings yet
- UMG Corporate ProfileDocument36 pagesUMG Corporate ProfileAnonymous 065EZLvNo ratings yet
- UNIV COM 2020-Match-Results PDFDocument5 pagesUNIV COM 2020-Match-Results PDFJHNo ratings yet
- Cover LetterDocument1 pageCover Letterapi-354128955No ratings yet
- Time, Final Rinse Protocol and EndodonticsDocument1 pageTime, Final Rinse Protocol and EndodonticsvaamdevaaNo ratings yet
- American Bar AssociationDocument6 pagesAmerican Bar AssociationMarkWarner100% (1)
- Hippocrates - W.hs. Jones 2.ciltDocument416 pagesHippocrates - W.hs. Jones 2.ciltmahmut sansalNo ratings yet
- Breach of Duty of Care in Medical Negligence: Scope and LimitationDocument55 pagesBreach of Duty of Care in Medical Negligence: Scope and LimitationNaina Mathew100% (1)
- Cayman Introduces Lateral Flow Tests for COVID StrategyDocument4 pagesCayman Introduces Lateral Flow Tests for COVID StrategyBrigita NemetNo ratings yet
- SIDDHA HERBAL MEDICINEDocument62 pagesSIDDHA HERBAL MEDICINEAnandan Arun100% (2)
- ANNEX A Masterlists of School Based Immunization 2019Document24 pagesANNEX A Masterlists of School Based Immunization 2019KRIZZIE JOY CAILINGNo ratings yet
- Preoperative PreparationDocument22 pagesPreoperative Preparationjackyploes100% (1)
- Simultaneous Treatment of Substance Abuse and Post-Traumatic Stress Disorder-A Case StudyDocument17 pagesSimultaneous Treatment of Substance Abuse and Post-Traumatic Stress Disorder-A Case StudyFedoxyzNo ratings yet