You might also like
- Gynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenFrom EverandGynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenNo ratings yet
- Recent Advancement in Infertility Management and Adoption ProcessDocument160 pagesRecent Advancement in Infertility Management and Adoption ProcessBhawna JoshiNo ratings yet
- Infertility - Definition, Causes, Diagnostic Procedures AND CouncellingDocument37 pagesInfertility - Definition, Causes, Diagnostic Procedures AND CouncellingvincentsharonNo ratings yet
- Diagnostic Tools in ObgynDocument27 pagesDiagnostic Tools in ObgynHenok Y KebedeNo ratings yet
- Infertility: Reshmi SibyDocument80 pagesInfertility: Reshmi SibySusan ThomasNo ratings yet
- Presented by DR - Shahbaz Ahmad Professor of Community MedicineDocument76 pagesPresented by DR - Shahbaz Ahmad Professor of Community MedicinePriya bhattiNo ratings yet
- Hormonal ContraceptivesDocument25 pagesHormonal Contraceptivesmd easarur rahmanNo ratings yet
- Monday PresentationsDocument20 pagesMonday PresentationsSunaina BhartiNo ratings yet
- Ca Cervix: DR Monika Teresa Prasetyo DR Sienny Amelia KwokDocument73 pagesCa Cervix: DR Monika Teresa Prasetyo DR Sienny Amelia KwokZien SienNo ratings yet
- Female Reproductive SystemDocument6 pagesFemale Reproductive SystemAlyanna L. ArquillanoNo ratings yet
- Pelvic Inflammatory Disease by SlidesgoDocument51 pagesPelvic Inflammatory Disease by SlidesgoGina MorenoNo ratings yet
- Infertility and Climacteric CrisisDocument4 pagesInfertility and Climacteric Crisisgeorgeloto12No ratings yet
- Mullarian AnomoliesDocument85 pagesMullarian AnomoliesPrathibha GuruguriNo ratings yet
- DR - Umpierrere2012 2013 4Document70 pagesDR - Umpierrere2012 2013 4Roberto RamosNo ratings yet
- Lesions of CervixDocument56 pagesLesions of Cervixvandana100% (1)
- Hysteroscopic Limitations PDFDocument59 pagesHysteroscopic Limitations PDFV R100% (1)
- Lesi Pra Kanker ServiksDocument34 pagesLesi Pra Kanker ServiksNeni SetyoNo ratings yet
- Medical and Surgical Management: of Uterine LeiomyomasDocument78 pagesMedical and Surgical Management: of Uterine LeiomyomasMarthinKolelupunNo ratings yet
- Premalignant Lesions of The Vulva and VaginaDocument42 pagesPremalignant Lesions of The Vulva and Vaginakaren carpioNo ratings yet
- Abnormal Uterine BleedingDocument39 pagesAbnormal Uterine BleedingVincentiusNo ratings yet
- 1 InroductionDocument44 pages1 Inroductiondemeke andebetNo ratings yet
- The Gonadal Hormones & Inhibitors: by M.H.Farjoo M.D., PH.DDocument133 pagesThe Gonadal Hormones & Inhibitors: by M.H.Farjoo M.D., PH.DsajidNo ratings yet
- Menopause Dan KlimakteriumDocument20 pagesMenopause Dan KlimakteriumAlfix AnugrahNo ratings yet
- Breast Cancer PowerpointDocument13 pagesBreast Cancer PowerpointCara DeaNo ratings yet
- Ectopic Pregnancy (Autosaved)Document56 pagesEctopic Pregnancy (Autosaved)susmita shresthaNo ratings yet
- Vulvovaginal Infections, Cervicitis and Bartholin's Cyst: Suparna Chhibber, MDDocument44 pagesVulvovaginal Infections, Cervicitis and Bartholin's Cyst: Suparna Chhibber, MDTeguh Imana NugrahaNo ratings yet
- Polycystic Ovarian Syndrome: Dr. PrabhavathiDocument30 pagesPolycystic Ovarian Syndrome: Dr. PrabhavathiKasi PrasadNo ratings yet
- Human Papillomavirus VaccineDocument18 pagesHuman Papillomavirus VaccineJarvis Guthrey BaldopeñaNo ratings yet
- MSN Seminar: Presenter-Miss. Nikhat KhanDocument35 pagesMSN Seminar: Presenter-Miss. Nikhat Khannikhat khanNo ratings yet
- Metabolic and Endocrine Pharmacology: Gonadol DrugsDocument38 pagesMetabolic and Endocrine Pharmacology: Gonadol Drugstheintrov100% (1)
- Laparoscopic Gynecologist Surgeon in HSR Layout BangaloreDocument8 pagesLaparoscopic Gynecologist Surgeon in HSR Layout BangaloreDr.Beena JeysinghNo ratings yet
- PHYSIOLOGY OF THE MENSTRUAL CYCLE بحث دكتوره ميDocument22 pagesPHYSIOLOGY OF THE MENSTRUAL CYCLE بحث دكتوره ميSoma Al-otaibyNo ratings yet
- Pap Smear Guidelines: Baylor College of Medicine Anoop Agrawal, M.DDocument22 pagesPap Smear Guidelines: Baylor College of Medicine Anoop Agrawal, M.Dshygirl72No ratings yet
- Management of Benign Breast Conditions: Part 2 - Breast Lumps and LesionsDocument3 pagesManagement of Benign Breast Conditions: Part 2 - Breast Lumps and Lesionspeter_mrNo ratings yet
- Ambulatory Hysteroscopy Evidence-Based Guide To Diagnosis and TherapyDocument23 pagesAmbulatory Hysteroscopy Evidence-Based Guide To Diagnosis and TherapyAngela EstevesNo ratings yet
- HysterosDocument17 pagesHysterosAnto PopaNo ratings yet
- Infertility IDocument36 pagesInfertility Idr_asaleh100% (1)
- Sexually Transmitted DiseasesDocument14 pagesSexually Transmitted DiseasesMartha P0% (1)
- Malignant Diseases of The CervixDocument128 pagesMalignant Diseases of The Cervixnicewan0% (1)
- Anatomy of Female Genital Tract by Sidra IftikharDocument33 pagesAnatomy of Female Genital Tract by Sidra IftikharWaqas Tahir100% (1)
- Dilation and CurettageDocument9 pagesDilation and CurettagedenekeNo ratings yet
- Biomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueDocument12 pagesBiomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueWahyuning PutriNo ratings yet
- Breast CancerDocument29 pagesBreast CancerJet-Jet GuillerganNo ratings yet
- Cervix Cancer Power Point With SlidesDocument41 pagesCervix Cancer Power Point With SlidesAmín JiménezNo ratings yet
- What Is The Differential Diagnosis For The Breast Mass in An Adolescent?Document4 pagesWhat Is The Differential Diagnosis For The Breast Mass in An Adolescent?theodore_estradaNo ratings yet
- Investigation InfertilityDocument44 pagesInvestigation InfertilityDenisNo ratings yet
- Obstetric Anal Sphincter Injury (OASIS) - UpToDateDocument39 pagesObstetric Anal Sphincter Injury (OASIS) - UpToDateErickNo ratings yet
- Pop QDocument45 pagesPop QObgyn Maret2016No ratings yet
- Endometrial Cancer: Manuela RussuDocument38 pagesEndometrial Cancer: Manuela RussuAnonymous 0XqZUl06PmNo ratings yet
- Your Breast Health: Presented By: Eric Lachman and Kim LeDocument23 pagesYour Breast Health: Presented By: Eric Lachman and Kim Leeric_lachman5234No ratings yet
- Management of Polycystic Ovary Syndrome in Case ofDocument18 pagesManagement of Polycystic Ovary Syndrome in Case ofMelati PratiwiNo ratings yet
- O&G Counselling - TSPDocument6 pagesO&G Counselling - TSPTarran PhagooNo ratings yet
- Abortion ..Document53 pagesAbortion ..Karan SinghNo ratings yet
- FIGO Cancer Report 2018 PDFDocument128 pagesFIGO Cancer Report 2018 PDFAndi Tiara S. AdamNo ratings yet
- Drugs 2 (Gyneac)Document103 pagesDrugs 2 (Gyneac)Aman Shaikh100% (2)
- Hysteroscopy Newsletter Vol 2 Issue 2 EnglishDocument23 pagesHysteroscopy Newsletter Vol 2 Issue 2 EnglishHisteroscopia.esNo ratings yet
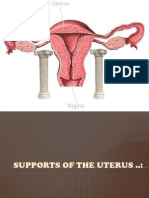
- Supports of The UterusDocument20 pagesSupports of The UterusAshwin Prem Solomon100% (1)
- Abnormal Uterine BleedingDocument5 pagesAbnormal Uterine Bleedingwuryan dewiNo ratings yet
- Spontaneous Vaginal Delivery IN Post Term PregnancyDocument55 pagesSpontaneous Vaginal Delivery IN Post Term Pregnancyr.pavinvikneshNo ratings yet
- Behavioural Issues Associated With Long Duration Expedition Missions - NASADocument116 pagesBehavioural Issues Associated With Long Duration Expedition Missions - NASAJp VillalonNo ratings yet
- Lab Assignment 3Document3 pagesLab Assignment 3Zack Zckz100% (1)
- Leaf Area Estimation of Anacardium HumileDocument8 pagesLeaf Area Estimation of Anacardium HumileAngelita SoaresNo ratings yet
- Calculus: Early Transcendental Functions 7th Edition by Ron Larson, Bruce H. Edwards Test Bank and Solution ManualDocument8 pagesCalculus: Early Transcendental Functions 7th Edition by Ron Larson, Bruce H. Edwards Test Bank and Solution ManualMiguel Tejeda0% (1)
- Best Python TutorialDocument32 pagesBest Python Tutorialnord vpn1No ratings yet
- Astrology & FoodDocument4 pagesAstrology & FoodTARATARINI COLLEGENo ratings yet
- Banking Financial InstitutionsDocument252 pagesBanking Financial Institutionspraise ferrerNo ratings yet
- Abu Ibrahim Al-Hashimi Al-Qurashi: Abū Ibrāhīm Al-Hāshimi Al-Qurashi Mawli Al-SalbiDocument12 pagesAbu Ibrahim Al-Hashimi Al-Qurashi: Abū Ibrāhīm Al-Hāshimi Al-Qurashi Mawli Al-SalbiJosué Barrón GonzálezNo ratings yet
- Code For VirtualboxDocument1 pageCode For VirtualboxAnonymous 4m8ueTNo ratings yet
- Aldabbagh 4417Document322 pagesAldabbagh 4417michael ballNo ratings yet
- Measurement of Hardness of Rubber CompoundsDocument8 pagesMeasurement of Hardness of Rubber CompoundsDarshan VariaNo ratings yet
- Coerver Training DrillsDocument5 pagesCoerver Training Drillsburvi200111860% (1)
- Tutorial ControlDocument161 pagesTutorial ControlQuangNguyenDuy100% (1)
- GBC Module 1Document69 pagesGBC Module 1MOHAMED82% (129)
- TOC - Building in TimeDocument3 pagesTOC - Building in Timemillerka2No ratings yet
- Your Initial Task. Find Out What's in Me!Document6 pagesYour Initial Task. Find Out What's in Me!Earl MontecastroNo ratings yet
- Front PageDocument5 pagesFront PageAnas AloyodanNo ratings yet
- PfroDocument4 pagesPfrobe3pNo ratings yet
- Islamic Private Debt Securities (Ipds)Document37 pagesIslamic Private Debt Securities (Ipds)Sara IbrahimNo ratings yet
- 0-IEC Standards ListDocument161 pages0-IEC Standards Listrasheed313No ratings yet
- Practical 9: Enthalpy Change of ReactionDocument4 pagesPractical 9: Enthalpy Change of ReactionJulia QistinaNo ratings yet
- Masoneilan 31000 Series Rotary Control ValvesDocument12 pagesMasoneilan 31000 Series Rotary Control ValvesJuan Manuel AcebedoNo ratings yet
- Health Benefits of Financial Inclusion A Literature ReviewDocument7 pagesHealth Benefits of Financial Inclusion A Literature Reviewl1wot1j1fon3No ratings yet
- Table of Specifications With Test in Science - Quarter 4 - (Week 3 and Week 4)Document4 pagesTable of Specifications With Test in Science - Quarter 4 - (Week 3 and Week 4)Sarah Jane Lagura Rele50% (2)
- Dokumen - Tips Strength of Materials 5691845f3ea8eDocument13 pagesDokumen - Tips Strength of Materials 5691845f3ea8eJay GeeNo ratings yet
- Alessandro Albanese - All Season CollectionDocument29 pagesAlessandro Albanese - All Season CollectionWilliam BourneNo ratings yet
- Tomato BankDocument67 pagesTomato Bankkmusatheek musatheekNo ratings yet
- Report Documentation Page: Major James R. VanceDocument26 pagesReport Documentation Page: Major James R. VanceQazma RarajNo ratings yet
- Vertical Immersion Pump VTP-BBFDocument23 pagesVertical Immersion Pump VTP-BBFmourinho2No ratings yet
- W1 8GEC 2A Readings in The Philippine History IPED ModuleDocument74 pagesW1 8GEC 2A Readings in The Philippine History IPED ModuleMico S. IglesiaNo ratings yet