You might also like
- Sepsis and Septic Shock GuidelinesfinalDocument51 pagesSepsis and Septic Shock GuidelinesfinalElteyb Nor eldaimNo ratings yet
- Diabetes Mellitus: DR Hiew Fu LiongDocument30 pagesDiabetes Mellitus: DR Hiew Fu LiongamminsaffriNo ratings yet
- Critical Care: Sepsis inDocument8 pagesCritical Care: Sepsis inNancy GRCNo ratings yet
- Infeksi Bedah & Surviving Sepsis ChampaignDocument22 pagesInfeksi Bedah & Surviving Sepsis ChampaignHafiz AlfarizieNo ratings yet
- S1.1 Ria Bandiara - Role Managemen Hypertension PKB 2019Document29 pagesS1.1 Ria Bandiara - Role Managemen Hypertension PKB 2019siputleletNo ratings yet
- HBV Easl 2017Document57 pagesHBV Easl 2017jessica100% (1)
- Materi - STBI Cedera Kepala Di ICU-JIH 2022 DR SetyoriniDocument40 pagesMateri - STBI Cedera Kepala Di ICU-JIH 2022 DR SetyoriniDudhutt TVNo ratings yet
- CKDMMM 150717231019 Lva1 App6892 PDFDocument47 pagesCKDMMM 150717231019 Lva1 App6892 PDFTabada NickyNo ratings yet
- Komplikasi Akut DM - Dr. RensaDocument42 pagesKomplikasi Akut DM - Dr. RensaLeonardus William KuswaraNo ratings yet
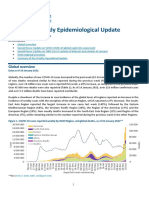
- COVID-19 Weekly Epidemiological Update: Global OverviewDocument16 pagesCOVID-19 Weekly Epidemiological Update: Global OverviewElia Nur IrmantiNo ratings yet
- Chronic Heart FailureDocument25 pagesChronic Heart FailureNeilavery WindaNo ratings yet
- EMERGENCIES IN DM (KAD Dan HHS)Document26 pagesEMERGENCIES IN DM (KAD Dan HHS)ozNo ratings yet
- Surviving Sepsis CampaignDocument16 pagesSurviving Sepsis CampaignKHAIRUL REDZUANNo ratings yet
- Spektrum AIDocument55 pagesSpektrum AIOgizWaraNo ratings yet
- WS 5 - DR DR C Heriawan Soejono, SPPD, KGer, M.Epid, MPH - TATALAKSANA PASIEN GERIATRI PDFDocument34 pagesWS 5 - DR DR C Heriawan Soejono, SPPD, KGer, M.Epid, MPH - TATALAKSANA PASIEN GERIATRI PDFApres SyahwaNo ratings yet
- Surving Sepsis 2021.anand - ErDocument74 pagesSurving Sepsis 2021.anand - ErbharatNo ratings yet
- GLOMERULOPATHYDocument51 pagesGLOMERULOPATHYAumnissa SamsiNo ratings yet
- J Jacc 2022 08 004Document171 pagesJ Jacc 2022 08 004Sur AJNo ratings yet
- Clinical Practice Guideline On Diagnosis and Treatment of Hyponatremia PDFDocument12 pagesClinical Practice Guideline On Diagnosis and Treatment of Hyponatremia PDFLuis Mochas HClNo ratings yet
- Pneumonia (Fix)Document64 pagesPneumonia (Fix)Kornelis AribowoNo ratings yet
- Diabetes IdiDocument71 pagesDiabetes IdiAriyanaNo ratings yet
- EMPEROR PreservedDocument38 pagesEMPEROR PreservedAppu Elias100% (1)
- Journal Reading Pneumoni Aspirasi - Kelompok 8Document21 pagesJournal Reading Pneumoni Aspirasi - Kelompok 8Rifly PradanaNo ratings yet
- GI Diseases Lecture on IBSDocument9 pagesGI Diseases Lecture on IBSEmeraldyModyNo ratings yet
- Anaphylaxis GuideDocument27 pagesAnaphylaxis Guidenadya idfentiNo ratings yet
- Biomarker Lactate (DR Agus Kosasih SPPK)Document31 pagesBiomarker Lactate (DR Agus Kosasih SPPK)sunterjaya1 sunterjaya1No ratings yet
- Mycobacterium Tuberculosis Complex & NtmsDocument4 pagesMycobacterium Tuberculosis Complex & NtmsCindy Mae Flores UtlegNo ratings yet
- Mayuri Thyroid MTDocument24 pagesMayuri Thyroid MTmayuri zanwarNo ratings yet
- Penyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUDocument56 pagesPenyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUFitriana WijayatiNo ratings yet
- Trulicity Webinar PAPDI Makassar 20 November 2021 MakbulDocument40 pagesTrulicity Webinar PAPDI Makassar 20 November 2021 MakbulNur Sabriany LihawaNo ratings yet
- AN AIDS PATIENT WITH CRYPTOCOCCUS NEOFORMANS PNEUMONIADocument26 pagesAN AIDS PATIENT WITH CRYPTOCOCCUS NEOFORMANS PNEUMONIABrinna Anindita SatriaNo ratings yet
- Acute Kidney InjuryDocument62 pagesAcute Kidney InjuryIvan HensonNo ratings yet
- PC Slides Packer - EMPEROR-ReducedDocument6 pagesPC Slides Packer - EMPEROR-ReducedSaul RuizNo ratings yet
- Pancreatic MalignancyDocument22 pagesPancreatic Malignancylovelots1234No ratings yet
- Inter'Medic CKDDocument31 pagesInter'Medic CKDMAHEJS HD100% (1)
- Emergency Medicine-Aru W. SudoyoDocument44 pagesEmergency Medicine-Aru W. SudoyoArdhiNo ratings yet
- FINAL Management Update of Hyperuricemia & GoutDocument50 pagesFINAL Management Update of Hyperuricemia & GoutNeni Septria NingsihNo ratings yet
- Pulmonary TuberculosisDocument38 pagesPulmonary TuberculosisHiba AssiNo ratings yet
- Jambore-Pkb (Lazuardi Dwipa, DR - SPPD, K-Ger)Document65 pagesJambore-Pkb (Lazuardi Dwipa, DR - SPPD, K-Ger)UPT PKM UJUNGBERUNG INDAHNo ratings yet
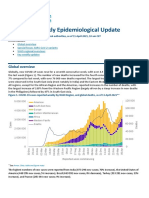
- COVID-19 Weekly Epidemiological Update: Global OverviewDocument31 pagesCOVID-19 Weekly Epidemiological Update: Global OverviewPaolaNo ratings yet
- Anemia in CKD and DialysisDocument38 pagesAnemia in CKD and Dialysisapoorva jainNo ratings yet
- DiureticsDocument61 pagesDiureticsJoyce WacukaNo ratings yet
- Consensus KDIGO ADADocument16 pagesConsensus KDIGO ADAAchrafNo ratings yet
- AsthmaDocument95 pagesAsthmaMohiuddin AhmedNo ratings yet
- Vilzap-M Synergy FlowDocument35 pagesVilzap-M Synergy FlowNimesh ModiNo ratings yet
- Venous Thromboemboly in Covid-19: DR. Dr. Idar Mappangara, SP - PD, SP - JP (K)Document30 pagesVenous Thromboemboly in Covid-19: DR. Dr. Idar Mappangara, SP - PD, SP - JP (K)haeriah sabaruddinNo ratings yet
- Szabo Michelle CV IptecDocument11 pagesSzabo Michelle CV Iptecapi-583778137No ratings yet
- Empa RegDocument49 pagesEmpa RegB ShahNo ratings yet
- A Review ThrombocytopeniaDocument5 pagesA Review ThrombocytopeniaEditor IJTSRDNo ratings yet
- Anestesi Bs Fix - Revisi (Edited)Document74 pagesAnestesi Bs Fix - Revisi (Edited)andi epri rangga adityaNo ratings yet
- Role of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy LestariDocument32 pagesRole of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy Lestaridesy lestariNo ratings yet
- Effects of Obesity On Infections With Emphasis On Skin Infections and Wound HealingDocument6 pagesEffects of Obesity On Infections With Emphasis On Skin Infections and Wound HealingFirdani Mutiara100% (1)
- PEMERIKSAAN LABORATORIUM UNTUK MONITORING INFEKSI HUMAN IMMUNODEFICIENCY VIRUSDocument33 pagesPEMERIKSAAN LABORATORIUM UNTUK MONITORING INFEKSI HUMAN IMMUNODEFICIENCY VIRUSMustakim DuharingNo ratings yet
- SSC 2021 GuidelinesDocument59 pagesSSC 2021 GuidelinesPrasannakumar P CNo ratings yet
- Tutorial Klinik Stase Ilmu Penyakit Dalam: GastrohepatologiDocument48 pagesTutorial Klinik Stase Ilmu Penyakit Dalam: GastrohepatologiMerry MiraNo ratings yet
- Pcol MidtermsDocument25 pagesPcol MidtermsnoyaNo ratings yet
- SEPSIS Early DetectionDocument35 pagesSEPSIS Early DetectionKomang_JananuragaNo ratings yet
- Surviving Sepsis Campaign Guideline: Managing Severe Sepsis and Septic ShockDocument38 pagesSurviving Sepsis Campaign Guideline: Managing Severe Sepsis and Septic ShockSelly RizanyNo ratings yet
- Sepsis Management GuidelinesDocument54 pagesSepsis Management Guidelinesfakhrina nur fadhillahNo ratings yet
- Gambaran Klinis Dan Tatalaksana SepsisDocument35 pagesGambaran Klinis Dan Tatalaksana SepsisyunielsyaNo ratings yet
- Gender-Based ViolenceDocument11 pagesGender-Based Violenceapi-581022439No ratings yet
- What To Do When Your Child Is Sick or HurtDocument1 pageWhat To Do When Your Child Is Sick or HurtWXYZ-TV Channel 7 DetroitNo ratings yet
- TCI Regiment - Candidate Medical FormDocument2 pagesTCI Regiment - Candidate Medical FormRichard Inoa JimenezNo ratings yet
- Practical PPT TDV Mod 2Document27 pagesPractical PPT TDV Mod 2Teja DvNo ratings yet
- Pathology (Awasir)Document152 pagesPathology (Awasir)Yousef TaqatqehNo ratings yet
- Obstructive Sleep Apnea in AdultsDocument2 pagesObstructive Sleep Apnea in AdultsElaine CristinaNo ratings yet
- Friday Seminar 9-23Document28 pagesFriday Seminar 9-23api-609125382No ratings yet
- 2208-147642 Embado Ma. LyraDocument1 page2208-147642 Embado Ma. LyraMarevic SanchezNo ratings yet
- ICU protocol 2015 قصر العيني by mansdocsDocument227 pagesICU protocol 2015 قصر العيني by mansdocsWalaa YousefNo ratings yet
- Biology Liver CirrhosisDocument15 pagesBiology Liver CirrhosisjohanstinNo ratings yet
- Vulvar Edema in Pregnancy A Case ReportDocument7 pagesVulvar Edema in Pregnancy A Case ReportNico PlantadoNo ratings yet
- The Body Dysmorphia Test - BDDFDocument1 pageThe Body Dysmorphia Test - BDDFNeven Č.No ratings yet
- HyperthermiaDocument5 pagesHyperthermiaCarey Jamille YadanNo ratings yet
- Materi Bahasa InggrisDocument3 pagesMateri Bahasa InggrisPaul JansenNo ratings yet
- NCP 1 AND SOAPIE 1) Ineffective Breathing PatternDocument5 pagesNCP 1 AND SOAPIE 1) Ineffective Breathing PatternMicaela CrisostomoNo ratings yet
- Approach To Joint Pain-1Document49 pagesApproach To Joint Pain-1Shivangi LodhaNo ratings yet
- Cabas GulayDocument44 pagesCabas GulayJamaicah CabasNo ratings yet
- Dsi Vs Rsi in TraumaDocument7 pagesDsi Vs Rsi in TraumaAbhi JeetNo ratings yet
- Chapter 27 Acute Lung Injury, Pulmonary Edema and Multi Organ System FailureDocument10 pagesChapter 27 Acute Lung Injury, Pulmonary Edema and Multi Organ System FailureShanin SalapuddinNo ratings yet
- Psychoeducation Barcelona ModelDocument12 pagesPsychoeducation Barcelona ModelAnnPSWNo ratings yet
- Acute Gingival InfectionsDocument45 pagesAcute Gingival InfectionsDUKUZIMANA CONCORDENo ratings yet
- Indian EconomyDocument10 pagesIndian Economyrajputdhruv100No ratings yet
- Pathophysiology NSTEMI 2022Document14 pagesPathophysiology NSTEMI 2022usmlesteveNo ratings yet
- SalmonellaDocument2 pagesSalmonellaAlfarizi Julistyo S.No ratings yet
- TB Screening and Diagnosis GuideDocument18 pagesTB Screening and Diagnosis GuideGloriana Julia TeopeNo ratings yet
- Family Violence in BangladeshDocument13 pagesFamily Violence in BangladeshFerdous MostofaNo ratings yet
- LEUKEMIA, MPDs & MDSsDocument11 pagesLEUKEMIA, MPDs & MDSsMary Kaye Yvonne OtillaNo ratings yet
- Blood TransfusionDocument5 pagesBlood TransfusionCYRIL YANNA MENDONESNo ratings yet
- Benign Convulsion With Mild GastroenteritisDocument6 pagesBenign Convulsion With Mild Gastroenteritisb101106036 TMUNo ratings yet
- Electro Convulsive Therapy (ECT)Document8 pagesElectro Convulsive Therapy (ECT)Lone SaithaNo ratings yet