You might also like
- Pharmacogenomics: From Discovery to Clinical ImplementationFrom EverandPharmacogenomics: From Discovery to Clinical ImplementationShowkat Ahmad GanieNo ratings yet
- Infeksi Bedah & Surviving Sepsis ChampaignDocument22 pagesInfeksi Bedah & Surviving Sepsis ChampaignHafiz AlfarizieNo ratings yet
- Diabetes Mellitus: DR Hiew Fu LiongDocument30 pagesDiabetes Mellitus: DR Hiew Fu LiongamminsaffriNo ratings yet
- Critical Care: Sepsis inDocument8 pagesCritical Care: Sepsis inNancy GRCNo ratings yet
- Komplikasi Akut DM - Dr. RensaDocument42 pagesKomplikasi Akut DM - Dr. RensaLeonardus William KuswaraNo ratings yet
- GI Diseases Lecture on IBSDocument9 pagesGI Diseases Lecture on IBSEmeraldyModyNo ratings yet
- Pancreatic MalignancyDocument22 pagesPancreatic Malignancylovelots1234No ratings yet
- CKDMMM 150717231019 Lva1 App6892 PDFDocument47 pagesCKDMMM 150717231019 Lva1 App6892 PDFTabada NickyNo ratings yet
- EMERGENCIES IN DM (KAD Dan HHS)Document26 pagesEMERGENCIES IN DM (KAD Dan HHS)ozNo ratings yet
- Diabetes IdiDocument71 pagesDiabetes IdiAriyanaNo ratings yet
- Anaphylaxis GuideDocument27 pagesAnaphylaxis Guidenadya idfentiNo ratings yet
- Disease of Adrenal Gland: Dr. Fatimah Eliana, SPPD, KemdDocument57 pagesDisease of Adrenal Gland: Dr. Fatimah Eliana, SPPD, KemdDeby Tri Widia LestariNo ratings yet
- Celiac DiseaseDocument25 pagesCeliac DiseaseMateen ShukriNo ratings yet
- Emergency Medicine-Aru W. SudoyoDocument44 pagesEmergency Medicine-Aru W. SudoyoArdhiNo ratings yet
- Dr. Erlieza Roosdhania, SP - PD (CKD)Document38 pagesDr. Erlieza Roosdhania, SP - PD (CKD)Pon PondNo ratings yet
- Epidemiologi, Klasifikasi, Diagnosis DMDocument75 pagesEpidemiologi, Klasifikasi, Diagnosis DMShibaNo ratings yet
- IPDIDocument30 pagesIPDIaris budionoNo ratings yet
- S1.1 Ria Bandiara - Role Managemen Hypertension PKB 2019Document29 pagesS1.1 Ria Bandiara - Role Managemen Hypertension PKB 2019siputleletNo ratings yet
- Surviving Sepsis CampaignDocument16 pagesSurviving Sepsis CampaignKHAIRUL REDZUANNo ratings yet
- AN AIDS PATIENT WITH CRYPTOCOCCUS NEOFORMANS PNEUMONIADocument26 pagesAN AIDS PATIENT WITH CRYPTOCOCCUS NEOFORMANS PNEUMONIABrinna Anindita SatriaNo ratings yet
- Tatalaksana Awal Koreksi Cairan pada Kasus SyokDocument60 pagesTatalaksana Awal Koreksi Cairan pada Kasus Syokmuhammad benyNo ratings yet
- Spektrum AIDocument55 pagesSpektrum AIOgizWaraNo ratings yet
- Diagnosa Dan Tatalaksana SepsisDocument51 pagesDiagnosa Dan Tatalaksana SepsisIndah apriliaNo ratings yet
- PansitopeniaDocument33 pagesPansitopeniaBrad WrightNo ratings yet
- Bimbingan Dokter Hari - CKDDocument24 pagesBimbingan Dokter Hari - CKDVicky LumalessilNo ratings yet
- BrucellosisDocument26 pagesBrucellosisVasilika GiemsaNo ratings yet
- Indonesia's Growing Diabetes EpidemicDocument28 pagesIndonesia's Growing Diabetes EpidemicAdhi TjahyadiNo ratings yet
- WS 5 - DR DR C Heriawan Soejono, SPPD, KGer, M.Epid, MPH - TATALAKSANA PASIEN GERIATRI PDFDocument34 pagesWS 5 - DR DR C Heriawan Soejono, SPPD, KGer, M.Epid, MPH - TATALAKSANA PASIEN GERIATRI PDFApres SyahwaNo ratings yet
- HBV Easl 2017Document57 pagesHBV Easl 2017jessica100% (1)
- TiroidDocument26 pagesTiroidJoni Riana MustaqimNo ratings yet
- REFERAT DMARDsDocument42 pagesREFERAT DMARDsBhayu Dharma SuryanaNo ratings yet
- Therapeutically Administered Ribonucleoside Analogue Mk-4482/Eidd-2801 Blocks Sars-Cov-2 Transmission in FerretsDocument15 pagesTherapeutically Administered Ribonucleoside Analogue Mk-4482/Eidd-2801 Blocks Sars-Cov-2 Transmission in FerretsCarlosgustavo SaavedrarubioNo ratings yet
- Surving Sepsis 2021.anand - ErDocument74 pagesSurving Sepsis 2021.anand - ErbharatNo ratings yet
- Modul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaDocument22 pagesModul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaYhaya 'Dzulhijjahyanti'No ratings yet
- The Brief Case Incidental Finding of Cystic Echinococcosis During Evaluation For HaematemesisDocument3 pagesThe Brief Case Incidental Finding of Cystic Echinococcosis During Evaluation For HaematemesisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integrated Medical Seminar Diabetes MellitusDocument33 pagesIntegrated Medical Seminar Diabetes MellitusKyo Jie MingNo ratings yet
- Program Pengendalian Resistensi Antimikroba Di Rumah SakitDocument23 pagesProgram Pengendalian Resistensi Antimikroba Di Rumah SakitYulia Wati Safitri SanjayaNo ratings yet
- Penyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUDocument56 pagesPenyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUFitriana WijayatiNo ratings yet
- Dr. Uun Sumardi, SPPD, K-PTI, KIC, FINASIM-Fluid Management in Severe DengueDocument20 pagesDr. Uun Sumardi, SPPD, K-PTI, KIC, FINASIM-Fluid Management in Severe DengueOlivia DwimaswastiNo ratings yet
- Intrapleural Ruptured Hydatid Cyst of Liver Presented As Eosinophilic Pleural Effusion: Case ReportDocument7 pagesIntrapleural Ruptured Hydatid Cyst of Liver Presented As Eosinophilic Pleural Effusion: Case ReportIJAR JOURNALNo ratings yet
- Bimbingan UKMPPD - IPDDocument50 pagesBimbingan UKMPPD - IPDlinggarNo ratings yet
- Geriatric Medicine KuliahDocument38 pagesGeriatric Medicine KuliahLia pramitaNo ratings yet
- Diabetes Melitus & PengelolaannyaDocument56 pagesDiabetes Melitus & PengelolaannyaIbnuNo ratings yet
- TK - Peran CA 125Document25 pagesTK - Peran CA 125Farli Wenang MaradjabessyNo ratings yet
- Hydatidosis: A Mystery Box at Various SitesDocument7 pagesHydatidosis: A Mystery Box at Various SitesIJAR JOURNALNo ratings yet
- Empagliflozin in Heart Failure With A Preserved Ejection FractionDocument11 pagesEmpagliflozin in Heart Failure With A Preserved Ejection Fractionsri wahyuniNo ratings yet
- Materi To Interna 02 FebruariDocument75 pagesMateri To Interna 02 FebruariMario AlexanderNo ratings yet
- Hepatorenal SyndromeDocument6 pagesHepatorenal SyndromeEveline YNo ratings yet
- Metabolic Disorders in Emergency OncologyDocument27 pagesMetabolic Disorders in Emergency Oncologytepat rshsNo ratings yet
- Bullous Pemphigoid Vs Epydermolysis Bullosa Acquisita: Diagnosis and How To DifferentiateDocument12 pagesBullous Pemphigoid Vs Epydermolysis Bullosa Acquisita: Diagnosis and How To DifferentiateIrene Irene100% (1)
- Acute Myocardial Infarction Causes and Clinical ManifestationsDocument2 pagesAcute Myocardial Infarction Causes and Clinical ManifestationsGun TargunaNo ratings yet
- Pulmonary TuberculosisDocument38 pagesPulmonary TuberculosisHiba AssiNo ratings yet
- Prof. Syakib Acute Kidney Injury - Internal Medicine Emergency Course - Agustus 2019-DikonversiDocument35 pagesProf. Syakib Acute Kidney Injury - Internal Medicine Emergency Course - Agustus 2019-DikonversidrroytambunanNo ratings yet
- Perioperative Management in Diabetes MellitusDocument20 pagesPerioperative Management in Diabetes MellitusChristopher RyalinoNo ratings yet
- Clinical Practice Guideline On Diagnosis and Treatment of Hyponatremia PDFDocument12 pagesClinical Practice Guideline On Diagnosis and Treatment of Hyponatremia PDFLuis Mochas HClNo ratings yet
- Bronchitis Acute and ChronicDocument3 pagesBronchitis Acute and Chronicdwi rina putriNo ratings yet
- Managing Febrile Neutropenia in Pediatric Oncology PatientsDocument38 pagesManaging Febrile Neutropenia in Pediatric Oncology Patientsdr FAHADKHALIQSIALNo ratings yet
- Chronic Liver DiseaseDocument3 pagesChronic Liver DiseaseMohammad AbbasNo ratings yet
- Jurding Nita Tka in RaDocument17 pagesJurding Nita Tka in RaNovitasariyantiNo ratings yet
- Surviving Sepsis Campaign: International Guidelines For Management of Sepsis and Septic Shock: 2016Document41 pagesSurviving Sepsis Campaign: International Guidelines For Management of Sepsis and Septic Shock: 2016Sarah OctavianiNo ratings yet
- Management of TB Special Cases: Presenter: Dr. Afaf AgeedDocument32 pagesManagement of TB Special Cases: Presenter: Dr. Afaf AgeedElteyb Nor eldaimNo ratings yet
- Basic Ventilation Guide: Intubation, Weaning, Modes & MoreDocument74 pagesBasic Ventilation Guide: Intubation, Weaning, Modes & MoreElteyb Nor eldaimNo ratings yet
- Icu Doing More Can Be WorseDocument6 pagesIcu Doing More Can Be WorsealinaNo ratings yet
- 4 5852862929099032890Document23 pages4 5852862929099032890Elteyb Nor eldaimNo ratings yet
- Diagnostic Accuracy of Pleural Fluid NT-Pro BNPDocument11 pagesDiagnostic Accuracy of Pleural Fluid NT-Pro BNPElteyb Nor eldaimNo ratings yet
- NullDocument58 pagesNullElteyb Nor eldaimNo ratings yet
- Managing COVID-19 Cases in the CommunityDocument18 pagesManaging COVID-19 Cases in the CommunityElteyb Nor eldaimNo ratings yet
- MF Taking Anticoagulation MedicineDocument5 pagesMF Taking Anticoagulation MedicineElteyb Nor eldaimNo ratings yet
- Bronchiectasis - AiimsrisDocument118 pagesBronchiectasis - AiimsrisElteyb Nor eldaimNo ratings yet
- Senior High School Tracks: Free Powerpoint Templates Free Powerpoint TemplatesDocument11 pagesSenior High School Tracks: Free Powerpoint Templates Free Powerpoint TemplatesGeraldineNo ratings yet
- Financial ManagementDocument2 pagesFinancial ManagementSanna KazmiNo ratings yet
- PhoneFreedom 365 0 Instalment Postpaid Phone Plan DigiDocument1 pagePhoneFreedom 365 0 Instalment Postpaid Phone Plan DigiJals JNo ratings yet
- My Watch Runs WildDocument3 pagesMy Watch Runs WildLarissa SnozovaNo ratings yet
- Twingo 3 & Clio 4Document10 pagesTwingo 3 & Clio 4Alexandre Le GrandNo ratings yet
- Mark Wildon - Representation Theory of The Symmetric Group (Lecture Notes) (2015)Document34 pagesMark Wildon - Representation Theory of The Symmetric Group (Lecture Notes) (2015)Satyam Agrahari0% (1)
- Lecture01 PushkarDocument27 pagesLecture01 PushkarabcdNo ratings yet
- Neutron SourcesDocument64 pagesNeutron SourcesJenodi100% (1)
- Sato Printer Api Reference DocumentDocument34 pagesSato Printer Api Reference Documentsupersteel.krwNo ratings yet
- A Report On Kantajew MandirDocument21 pagesA Report On Kantajew MandirMariam Nazia 1831388030No ratings yet
- Coffee TestDocument6 pagesCoffee TestAmit Satyen RaviNo ratings yet
- Transformers Obj Questions PDFDocument8 pagesTransformers Obj Questions PDFphaniputta100% (2)
- DataSheet IMA18-10BE1ZC0K 6041793 enDocument8 pagesDataSheet IMA18-10BE1ZC0K 6041793 enRuben Hernandez TrejoNo ratings yet
- TLM4ALL@1 Number System (EM)Document32 pagesTLM4ALL@1 Number System (EM)jkc collegeNo ratings yet
- Samsung RAM Product Guide Feb 11Document24 pagesSamsung RAM Product Guide Feb 11Javed KhanNo ratings yet
- Definition and Scope of Public FinanceDocument2 pagesDefinition and Scope of Public FinanceArfiya MubeenNo ratings yet
- Intermediate Accounting 2 - CL NCL Lecture NotesDocument2 pagesIntermediate Accounting 2 - CL NCL Lecture NotesRacheel SollezaNo ratings yet
- AP Standard Data All PDFDocument963 pagesAP Standard Data All PDFSiva Kumar100% (1)
- Temenos Brochure - FormpipeDocument5 pagesTemenos Brochure - FormpipeDanial OngNo ratings yet
- Joe Ann MarcellanaDocument17 pagesJoe Ann MarcellanarudyNo ratings yet
- Draconis CombineDocument11 pagesDraconis CombineMarco Moracha100% (1)
- Compare The Political System of Kazakhstan, USA, UK PresentationDocument19 pagesCompare The Political System of Kazakhstan, USA, UK PresentationAiganym OmiraliNo ratings yet
- FIL M 216 2nd Yer Panitikan NG PilipinasDocument10 pagesFIL M 216 2nd Yer Panitikan NG PilipinasJunas LopezNo ratings yet
- HFH ch04Document11 pagesHFH ch04Harikrishan RNo ratings yet
- LETTER OF AUTHORIZATION CREDO INVEST DownloadDocument1 pageLETTER OF AUTHORIZATION CREDO INVEST DownloadEsteban Enrique Posan BalcazarNo ratings yet
- Tle 10 4quarterDocument2 pagesTle 10 4quarterCaryll BaylonNo ratings yet
- Shooting ScriptDocument12 pagesShooting Scriptapi-544851273No ratings yet
- Kidney, bladder & prostate pathology slides explainedDocument20 pagesKidney, bladder & prostate pathology slides explainedNisrina Nur AzisahNo ratings yet
- St. Anthony College Calapan City Syllabus: Course DescriptionDocument6 pagesSt. Anthony College Calapan City Syllabus: Course DescriptionAce HorladorNo ratings yet
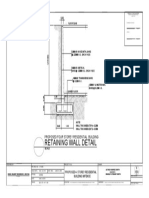
- Retaining Wall DetailsDocument1 pageRetaining Wall DetailsWilbert ReuyanNo ratings yet