You might also like
- Vesicovaginal FistulaDocument7 pagesVesicovaginal Fistuladrnareshkumar3281No ratings yet
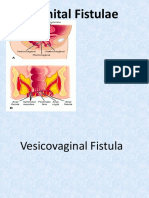
- Genital FistulaeDocument15 pagesGenital Fistulaesangeetha francisNo ratings yet
- Genito-Urinary Fistulas: Yashar Najiaghdam M.DDocument33 pagesGenito-Urinary Fistulas: Yashar Najiaghdam M.DRahul ChopadeNo ratings yet
- Hysterectomy 160819044047Document36 pagesHysterectomy 160819044047Baljeet KaurNo ratings yet
- Genital Tract InjuriesDocument74 pagesGenital Tract InjuriesDevuchandana RNo ratings yet
- Perineal TearsDocument44 pagesPerineal TearsMagic_OverNo ratings yet
- Genito-Urinary Fistulas: Yashar Najiaghdam M.DDocument33 pagesGenito-Urinary Fistulas: Yashar Najiaghdam M.DyoghaNo ratings yet
- Dilatation & Curettage: DR Ayswarya NarayanDocument19 pagesDilatation & Curettage: DR Ayswarya NarayanPrajwal Kp0% (1)
- Genitourinary Fistulas: Causes, Types, Diagnosis and ManagementDocument33 pagesGenitourinary Fistulas: Causes, Types, Diagnosis and ManagementDzulRizkaNo ratings yet
- Obstetric FistulaDocument52 pagesObstetric FistulaAdaiah Priscillia SoibiharryNo ratings yet
- Cesarean Section: Associate Professor Ph.D. E.A. EinyshDocument33 pagesCesarean Section: Associate Professor Ph.D. E.A. EinyshPrerit Aggarwal100% (1)
- Genito-Urinary FistulaDocument33 pagesGenito-Urinary Fistuladr_asaleh100% (4)
- Fistula GenitaliaDocument35 pagesFistula GenitaliaFifi FruitasariNo ratings yet
- Vesicovaginal Fistula: Urology DepartmentDocument24 pagesVesicovaginal Fistula: Urology DepartmentHardiTariqHamma100% (1)
- Bartholin's Gland CystDocument26 pagesBartholin's Gland Cystninjahattori1100% (1)
- Perianal Abscess - Pilonidal DiseaseDocument50 pagesPerianal Abscess - Pilonidal DiseaseAnonymous pTQIbWT2i9No ratings yet
- Anal Fistula Dont DeleteDocument28 pagesAnal Fistula Dont DeleteRazeen RiyasatNo ratings yet
- 10-Advance Nursing Management of Reproductive DiseasesDocument87 pages10-Advance Nursing Management of Reproductive Diseasesabdul satar100% (1)
- Micturating Cysto UrethrogramDocument33 pagesMicturating Cysto Urethrogramsabrinabari mohona35No ratings yet
- Permanent ContraceptionDocument33 pagesPermanent Contraceptionshyama seerviNo ratings yet
- Myomectomy Procedure OverviewDocument55 pagesMyomectomy Procedure Overviewchandani pandeyNo ratings yet
- Rectum Anatomy and Physiology Clinical FeaturesDocument36 pagesRectum Anatomy and Physiology Clinical FeaturesUsmle GuyNo ratings yet
- Surgery OsceDocument69 pagesSurgery OsceRebecca BrandonNo ratings yet
- Endometrial BiopsyDocument13 pagesEndometrial BiopsyChanta MaharjanNo ratings yet
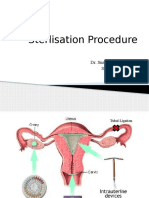
- Sterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalDocument30 pagesSterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalsushrutaNo ratings yet
- Obstetric Fistulae and Gynatresia Causes, Symptoms, and TreatmentDocument24 pagesObstetric Fistulae and Gynatresia Causes, Symptoms, and TreatmentnyangaraNo ratings yet
- Uterovaginal Prolapse Treatment OptionsDocument34 pagesUterovaginal Prolapse Treatment OptionskhadeejakhurshidNo ratings yet
- 5.fistula 29.7.19Document19 pages5.fistula 29.7.19HEZILNo ratings yet
- Reproductive Tract FistulaeDocument16 pagesReproductive Tract FistulaeKiprotich Titus NgetichNo ratings yet
- ProlapseDocument51 pagesProlapsejijaniNo ratings yet
- Urinary CatheterizationDocument41 pagesUrinary CatheterizationSteffiNo ratings yet
- Condom Balloon Controls Postpartum HemorrhageDocument50 pagesCondom Balloon Controls Postpartum HemorrhageBambang SulistyoNo ratings yet
- Obstetric FistulaDocument40 pagesObstetric Fistulamussahemed8No ratings yet
- Burst Abdomen Causes and TreatmentDocument15 pagesBurst Abdomen Causes and Treatmentsuhaibrehaman100% (1)
- UrethralstricturesDocument37 pagesUrethralstricturesNinaNo ratings yet
- Questions for the oral part of the practical skills examDocument22 pagesQuestions for the oral part of the practical skills examLucas Victor AlmeidaNo ratings yet
- RGU and MCU PPT Final For 18.9.23, BsmmuDocument46 pagesRGU and MCU PPT Final For 18.9.23, BsmmuMd.AlauddinNo ratings yet
- The Incompetent Cervix 2Document30 pagesThe Incompetent Cervix 2api-3705046100% (3)
- Vesico-vaginal fistula repairDocument8 pagesVesico-vaginal fistula repairBinita ShakyaNo ratings yet
- Repro Female Repro DisordersDocument11 pagesRepro Female Repro Disordersloli popNo ratings yet
- SurgeryDocument25 pagesSurgeryjackNo ratings yet
- Evidence Based Practices in ObstetricsDocument46 pagesEvidence Based Practices in Obstetricsvikas takNo ratings yet
- CystosDocument19 pagesCystosneenuj_5No ratings yet
- Management of Urological FistulaeDocument31 pagesManagement of Urological FistulaeBrendan DiasNo ratings yet
- Ecc Class 113 Pediatric Genitourinary DisordersDocument50 pagesEcc Class 113 Pediatric Genitourinary DisordersDinabandhu BaradNo ratings yet
- Suprapubic Cateterization Andrie Rev 2Document37 pagesSuprapubic Cateterization Andrie Rev 2Dwiyanti OktaviaNo ratings yet
- Benign Anorectal Surgical Disorders: Presenter: Kerubo MosetiDocument60 pagesBenign Anorectal Surgical Disorders: Presenter: Kerubo MosetiRisky OpponentNo ratings yet
- Total Laparoscopic Hysterectomy: Andrew Doering Minimally Invasive Surgery Lab University of KentuckyDocument32 pagesTotal Laparoscopic Hysterectomy: Andrew Doering Minimally Invasive Surgery Lab University of KentuckyJunaida AfifaNo ratings yet
- Abnormalities in Vagina and VulvaDocument32 pagesAbnormalities in Vagina and VulvaNovia RizqiNo ratings yet
- Burstabdomen 151223101029Document24 pagesBurstabdomen 151223101029ArifHidayatNo ratings yet
- Diaphragmatic Hernia Repair TechniquesDocument22 pagesDiaphragmatic Hernia Repair TechniquesAnmol SinghNo ratings yet
- Repro System NotesDocument13 pagesRepro System NotesAraw GabiNo ratings yet
- Birth Canal Injuries LectureDocument44 pagesBirth Canal Injuries LectureDeepali ThoratNo ratings yet
- Anorectal MalformationsDocument24 pagesAnorectal MalformationsVaishali SinghNo ratings yet
- Urinary Tract Infections (Utis) : Laboratory of Microbiology Medical Faculty Brawijaya UniversityDocument32 pagesUrinary Tract Infections (Utis) : Laboratory of Microbiology Medical Faculty Brawijaya UniversityMuhammad Ary R ANo ratings yet
- Bladder DiverticulaDocument23 pagesBladder DiverticulaJeanette CallejasNo ratings yet
- 0000 Recto-Vaginal Fistula 1Document11 pages0000 Recto-Vaginal Fistula 1Igwe SolomonNo ratings yet
- Puerperal Infections: Mrs - Jagadeeswari.J M.SC (N)Document43 pagesPuerperal Infections: Mrs - Jagadeeswari.J M.SC (N)Vincent Maralit MaterialNo ratings yet
- Genitourinary Fistulas GuideDocument46 pagesGenitourinary Fistulas GuidePrabhakar KumarNo ratings yet
- Catheter Care PlanDocument5 pagesCatheter Care PlanDilsha GurugeNo ratings yet
- Removing Indwelling CatheterDocument1 pageRemoving Indwelling CatheterAngelie PantajoNo ratings yet
- Cauda Equina Syndrome: A Simple Entity With Lot of Enigma!: EditorialDocument3 pagesCauda Equina Syndrome: A Simple Entity With Lot of Enigma!: EditorialsalikaabrarNo ratings yet
- Paediatrics - Urinary Tract Infection in Children PDFDocument5 pagesPaediatrics - Urinary Tract Infection in Children PDFJanelle NarcisoNo ratings yet
- Male CatheterizationDocument37 pagesMale CatheterizationJean Rynne BongaisNo ratings yet
- Nursing Education on CatheterizationDocument10 pagesNursing Education on CatheterizationPrasann RoyNo ratings yet
- Sign and Symptoms in Urology 1Document15 pagesSign and Symptoms in Urology 1Sri PertiwiNo ratings yet
- PSW - Employment Test Questionnaire - EMI32WBDocument5 pagesPSW - Employment Test Questionnaire - EMI32WBMonizaBorgesNo ratings yet
- Step-by-Step Guide to Bladder UltrasoundDocument24 pagesStep-by-Step Guide to Bladder Ultrasoundskype72214No ratings yet
- KistokelDocument4 pagesKistokelIntan PermataNo ratings yet
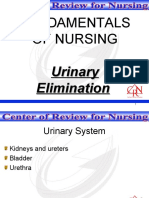
- Fundamentals of Nursing: Urinary EliminationDocument26 pagesFundamentals of Nursing: Urinary EliminationFEVIE ANNE BANATAONo ratings yet
- SIP (Paragis Plant)Document2 pagesSIP (Paragis Plant)Jazzy ArrezaNo ratings yet
- Acog Incontinencia Urinaria 2015Document16 pagesAcog Incontinencia Urinaria 2015amparoNo ratings yet
- BEDWETTING CAUSES AND TREATMENTSDocument3 pagesBEDWETTING CAUSES AND TREATMENTSPrincess Angel LucanasNo ratings yet
- Hii PDFDocument4 pagesHii PDFSydney VellaNo ratings yet
- Breakthrough Pelvic Pain Report - REBALANCE PTDocument13 pagesBreakthrough Pelvic Pain Report - REBALANCE PTSyed iliyasNo ratings yet
- Comite 20 PDFDocument124 pagesComite 20 PDFFelicia WagnerNo ratings yet
- Color and Label The Urinary SystemDocument1 pageColor and Label The Urinary Systemkurucz barbaraNo ratings yet
- Functional Status Assessment ReportDocument1 pageFunctional Status Assessment ReporttaisoNo ratings yet
- Neurogenic BladderDocument11 pagesNeurogenic BladderRoy LiemNo ratings yet
- Urinary SystemDocument10 pagesUrinary SystemMaruen RodriguezNo ratings yet
- CatheterizationDocument3 pagesCatheterization1H - Althea VestilNo ratings yet
- Urogynecology Examination: Divisi Uroginekologi Rekonstruksi Departemen Obstetri Dan Ginekologi Fkui/ RSCMDocument19 pagesUrogynecology Examination: Divisi Uroginekologi Rekonstruksi Departemen Obstetri Dan Ginekologi Fkui/ RSCMjuanda raynaldi100% (1)
- The Coombe Physiotherapy & Your Pelvic Floor Feb 2021Document20 pagesThe Coombe Physiotherapy & Your Pelvic Floor Feb 2021Andreea ManeaNo ratings yet
- Best Treatments For An Overactive BladderDocument11 pagesBest Treatments For An Overactive BladderJimmy GillNo ratings yet
- Urinary Catheter Types and Care For Residents With CathetersDocument10 pagesUrinary Catheter Types and Care For Residents With CathetersCarmen T OrtizNo ratings yet
- FBCDocument14 pagesFBCJane GarciaNo ratings yet
- Colostomy Care and IrrigationDocument6 pagesColostomy Care and IrrigationTheSweetpea501No ratings yet
- Welcome To Presentation: Presented by Karishma Mahato Roll No. 15Document18 pagesWelcome To Presentation: Presented by Karishma Mahato Roll No. 15sushma shresthaNo ratings yet
- Elvic Floor Muscle Activity in Different Sitting Postures in Continent and Incontinent Women - Sa - 0Document7 pagesElvic Floor Muscle Activity in Different Sitting Postures in Continent and Incontinent Women - Sa - 0Pollyana Furtado JunqueiraNo ratings yet