You might also like
- Amplivox CA850 Series 3 Operating Manual Issue 11Document26 pagesAmplivox CA850 Series 3 Operating Manual Issue 11PraistonNo ratings yet
- YALE (D879) GLC155VX LIFT TRUCK Service Repair Manual PDFDocument35 pagesYALE (D879) GLC155VX LIFT TRUCK Service Repair Manual PDFjkdmsmemmd67% (3)
- Ofs Qhse Quest 1 NewDocument78 pagesOfs Qhse Quest 1 Newhicham_080% (2)
- HD 050 Slidebar ManualDocument50 pagesHD 050 Slidebar ManualMarco Vinicio BazzottiNo ratings yet
- Loan Kit Management Information PackDocument21 pagesLoan Kit Management Information Packgadhang dewanggaNo ratings yet
- PDF pt203 Sos Nutanix TroubleshootingDocument26 pagesPDF pt203 Sos Nutanix TroubleshootingAdiWidyantoNo ratings yet
- Root Cause Analysis PresentationDocument37 pagesRoot Cause Analysis PresentationucheonixNo ratings yet
- Root Cause Analysis (RCA)Document153 pagesRoot Cause Analysis (RCA)Solha89% (9)
- Step Guide To Protocol Based CareDocument19 pagesStep Guide To Protocol Based CareAbdus Subhan A TakildarNo ratings yet
- BA 635 Disaster Recovery Research Paper - JitendraDocument12 pagesBA 635 Disaster Recovery Research Paper - Jitendraanchal singh100% (1)
- 16M Motor Grader-Maintenance IntervalsDocument62 pages16M Motor Grader-Maintenance IntervalsJuan Amanqui Garcia100% (3)
- Root Cause Analysis (RCA) : Grace Gwe-Ya Kim, PH.DDocument36 pagesRoot Cause Analysis (RCA) : Grace Gwe-Ya Kim, PH.DPeterNo ratings yet
- Root Cause Analysis ToolsDocument7 pagesRoot Cause Analysis ToolsSofiane IdjerNo ratings yet
- Cycle 1 - DR Ashutosh SarwaDocument17 pagesCycle 1 - DR Ashutosh Sarwajeena pradeepNo ratings yet
- Guide To Quality Assurance PlansDocument67 pagesGuide To Quality Assurance PlansMukeshNo ratings yet
- CIStandards Steps1 10 V2rev08302016 2Document2 pagesCIStandards Steps1 10 V2rev08302016 2Are Em GeeNo ratings yet
- Root Cause Analysis Template 22Document9 pagesRoot Cause Analysis Template 22Devi ChintyaNo ratings yet
- Root Cause Analysis Template 1Document11 pagesRoot Cause Analysis Template 1benaoumeur benouna100% (1)
- AGL Interview Case Study 2 SolutionDocument8 pagesAGL Interview Case Study 2 SolutionyomolojaNo ratings yet
- Non-Intrusive Inspection (NII) of Offshore Process Vessels (CAS132a)Document2 pagesNon-Intrusive Inspection (NII) of Offshore Process Vessels (CAS132a)Mario MeloNo ratings yet
- Corrective Action AND Preventive ActionDocument42 pagesCorrective Action AND Preventive Actionkevinwz1989No ratings yet
- 189382.visual Guide To PaperDocument10 pages189382.visual Guide To PaperAbdul AwanNo ratings yet
- Lecture 03 - Resources and Requirements For The IAEA Remote QC Program FINALDocument24 pagesLecture 03 - Resources and Requirements For The IAEA Remote QC Program FINALRoshi_11No ratings yet
- Root Cause Analysis Template PDFDocument6 pagesRoot Cause Analysis Template PDFRatish Nair100% (1)
- Title: Root Cause Evaluation Manual: ApprovalDocument10 pagesTitle: Root Cause Evaluation Manual: ApprovalMari LizNo ratings yet
- Iso22000 2005Document48 pagesIso22000 2005STELLA MARISNo ratings yet
- Industry Case Study Continued Process Verification CPV For A Biotech Product PDFDocument43 pagesIndustry Case Study Continued Process Verification CPV For A Biotech Product PDFPatricia Joyce Malabanan Sunglao100% (1)
- ISOH Presentation - PHNIGDocument45 pagesISOH Presentation - PHNIGDanOtah100% (1)
- Dxa Quality AssuranceDocument54 pagesDxa Quality AssuranceLinh BuiNo ratings yet
- INTERTANKO Vetting Committee 26.05.2022Document29 pagesINTERTANKO Vetting Committee 26.05.2022soner100% (1)
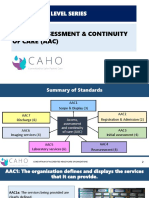
- AAC-Entry Level SeriesDocument51 pagesAAC-Entry Level SeriesPallavi Deepak DongreNo ratings yet
- Root Cause AnalysisDocument65 pagesRoot Cause Analysissyed ali mesum rizviNo ratings yet
- Iqpacs Radivision DCFDocument42 pagesIqpacs Radivision DCFtretdgdNo ratings yet
- Slickline Fishing Training - Client Course Agenda & TimetableDocument3 pagesSlickline Fishing Training - Client Course Agenda & TimetableEduardo OyarzunNo ratings yet
- Imp SsibundleDocument41 pagesImp SsibundlePPI Rs Dewi SriNo ratings yet
- TQCs For The Indirect Channel V1.3Document10 pagesTQCs For The Indirect Channel V1.3Edward Jose Cardenas CamachoNo ratings yet
- Root Cause Analysis Tool (RCAT)Document13 pagesRoot Cause Analysis Tool (RCAT)Jean CostaNo ratings yet
- Auvsi / Onr Student AUV CompetitionDocument33 pagesAuvsi / Onr Student AUV CompetitionPoondla PrashantNo ratings yet
- Clinauditchap 2Document22 pagesClinauditchap 2Goodness AjaeroNo ratings yet
- Stuart Wright Capability Feb 21Document19 pagesStuart Wright Capability Feb 21Julian Barrero MontalvoNo ratings yet
- Introduction To Kaizen Pdca ReportingDocument43 pagesIntroduction To Kaizen Pdca ReportingAiman DanishNo ratings yet
- RCA FinalDocument47 pagesRCA FinalSelvaraj S100% (1)
- Nerc 101Document124 pagesNerc 101VanNo ratings yet
- AZANFACK Helina Presentation IntegrationofPatientInformationSystemwithPictureArchiving AzanfDocument25 pagesAZANFACK Helina Presentation IntegrationofPatientInformationSystemwithPictureArchiving AzanffernandoNo ratings yet
- Brkewn 3011 PDFDocument126 pagesBrkewn 3011 PDFprakashrjsekarNo ratings yet
- VAN High Level DesignDocument36 pagesVAN High Level DesignMusariri TalentNo ratings yet
- Factor Criteria Observation Recommendation: Element No 1Document7 pagesFactor Criteria Observation Recommendation: Element No 1Emmanuel BatinganNo ratings yet
- An Overview of The Petroleum Resources Management System: and Its Relationship To UNFCDocument23 pagesAn Overview of The Petroleum Resources Management System: and Its Relationship To UNFCachmad.No ratings yet
- Confab SB 2016 Rev3pptxDocument15 pagesConfab SB 2016 Rev3pptxjaonnNo ratings yet
- AUDITING Internal Controls - 2024Document30 pagesAUDITING Internal Controls - 2024lonaarbillyNo ratings yet
- Root Cause FailureDocument14 pagesRoot Cause FailureRajAnandNo ratings yet
- Lecture 04 - The Added Value of Remote Automated QC at The Clinical Setting DraftDocument15 pagesLecture 04 - The Added Value of Remote Automated QC at The Clinical Setting DraftRoshi_11No ratings yet
- Presentation 7 - How To Conduct Cleaner Production Assessments? 1Document44 pagesPresentation 7 - How To Conduct Cleaner Production Assessments? 1GokulNo ratings yet
- Pipeline Asset IntegrityDocument41 pagesPipeline Asset IntegrityAkhil Joseph100% (1)
- Lecture 01 - Framework of Remote Automated QC FINALDocument18 pagesLecture 01 - Framework of Remote Automated QC FINALRoshi_11No ratings yet
- Wa0006Document8 pagesWa0006api-530767316No ratings yet
- Xpert QA Guide 2019Document92 pagesXpert QA Guide 2019falberto.gutierrezNo ratings yet
- 10 Steps To Asset CareDocument13 pages10 Steps To Asset CareDamianNo ratings yet
- Unit 4: Quality Control and Inspection: Programme Code-MeDocument32 pagesUnit 4: Quality Control and Inspection: Programme Code-Mesamirgaurave5No ratings yet
- Nuclear Maintenance Applications Center - Preventive Maintenance Program Guideline - Composite FlowchartDocument12 pagesNuclear Maintenance Applications Center - Preventive Maintenance Program Guideline - Composite FlowchartErwin Olav Ecos TovarNo ratings yet
- QA-QC Document E&I - 4Document103 pagesQA-QC Document E&I - 4M.sadaNo ratings yet
- Pedoman RCADocument16 pagesPedoman RCARonald Cyg DiaNo ratings yet
- Anpqp Version 2 1 - Accompagnateur - Day 1 On 2 - 251108Document96 pagesAnpqp Version 2 1 - Accompagnateur - Day 1 On 2 - 251108adrianNo ratings yet
- Life-Cycle Costing: Using Activity-Based Costing and Monte Carlo Methods to Manage Future Costs and RisksFrom EverandLife-Cycle Costing: Using Activity-Based Costing and Monte Carlo Methods to Manage Future Costs and RisksNo ratings yet
- Analysis Within the Systems Development Life-Cycle: Book 2 Data Analysis — The MethodsFrom EverandAnalysis Within the Systems Development Life-Cycle: Book 2 Data Analysis — The MethodsNo ratings yet
- Spaulding Classification SystemDocument1 pageSpaulding Classification Systempatel bhaumikNo ratings yet
- Ventilator Associated Event SurveillanceDocument32 pagesVentilator Associated Event Surveillancepatel bhaumikNo ratings yet
- Bachyryczimmunize Wise 2021FINALFINALUPDATEDocument44 pagesBachyryczimmunize Wise 2021FINALFINALUPDATEpatel bhaumikNo ratings yet
- Hospital Acquired InfectionsDocument64 pagesHospital Acquired Infectionspatel bhaumikNo ratings yet
- 09 Urinary Tract Infections in The ElderlyDocument19 pages09 Urinary Tract Infections in The Elderlypatel bhaumikNo ratings yet
- FPE REPORT Sugarcane JuiceDocument21 pagesFPE REPORT Sugarcane JuiceAini SyakirahNo ratings yet
- Rethinking The Evaluation For Conversational Recommendation in The Era of Large Language ModelsDocument19 pagesRethinking The Evaluation For Conversational Recommendation in The Era of Large Language Modelscynorr rainNo ratings yet
- Research Proposal Assignment Nguyen Van Khoa 12aDocument11 pagesResearch Proposal Assignment Nguyen Van Khoa 12aruacon_stevenNo ratings yet
- Modern Control System TutorialDocument134 pagesModern Control System TutorialUtn LeoNo ratings yet
- Science Experiment 1Document5 pagesScience Experiment 1Ameir Adha93% (14)
- Mengetik Arab Menggunakan Microsoft Office 2007Document8 pagesMengetik Arab Menggunakan Microsoft Office 2007alfeddsNo ratings yet
- PDS SikaTherm 4225 eDocument2 pagesPDS SikaTherm 4225 eMarian ComaniciNo ratings yet
- Chapter III - 1.2 Solution of The Assignment ModelDocument24 pagesChapter III - 1.2 Solution of The Assignment ModelMiks EnriquezNo ratings yet
- Wireless Communications MCQDocument20 pagesWireless Communications MCQRenisha BennoNo ratings yet
- Autonomous Database 100 PDFDocument36 pagesAutonomous Database 100 PDFLesile DiezNo ratings yet
- Eco162 104Document12 pagesEco162 104Abdullah RamlyNo ratings yet
- Maruti SuzukiDocument2 pagesMaruti SuzukiSneha SreekumarNo ratings yet
- ReadmeDocument3 pagesReadmeAlejandro MagnoNo ratings yet
- National Transmission Corp. v. de Jesus PDFDocument4 pagesNational Transmission Corp. v. de Jesus PDFJerald Oliver Macabaya0% (1)
- 19 Businesses Without Capital PDFDocument40 pages19 Businesses Without Capital PDFPreciousNo ratings yet
- #SM4J Recap Fall 2019Document5 pages#SM4J Recap Fall 2019Damian RadcliffeNo ratings yet
- Stepper Motor Speed Control 1Document8 pagesStepper Motor Speed Control 1Mahesh kumarNo ratings yet
- Automatic Rain Operated Wiper System in Automobile: A ReviewDocument3 pagesAutomatic Rain Operated Wiper System in Automobile: A ReviewAkarsh AdiNo ratings yet
- The Ability To Read and Write.: Media The Physical Objects Used To Communicate With, or The Mass CommunicationDocument3 pagesThe Ability To Read and Write.: Media The Physical Objects Used To Communicate With, or The Mass CommunicationRachel MonesNo ratings yet
- Wip Osp SetupDocument3 pagesWip Osp SetupMohan Kumar NagalingamNo ratings yet
- PHIL - Am Application Letter and Guidelines For PracticumDocument2 pagesPHIL - Am Application Letter and Guidelines For PracticumCristine CempronNo ratings yet
- 118: The Mill, Llanddewi Skirrid, Abergavenny. Watching BriefDocument20 pages118: The Mill, Llanddewi Skirrid, Abergavenny. Watching BriefAPAC LtdNo ratings yet
- Name of Employee: - PositionDocument1 pageName of Employee: - PositionAvery Jan Magabanua SilosNo ratings yet
- SOAP POI Web Service Reference PDFDocument11 pagesSOAP POI Web Service Reference PDFeko_suwarsonoNo ratings yet
- Kentucky Fried Chicken KFC Marketing Mix Four PsDocument25 pagesKentucky Fried Chicken KFC Marketing Mix Four PsRahul Singh RathoreNo ratings yet