You might also like
- Shock: Dr. P. Manoj Kumar Asst. Professor, Dep. of Gen. Surgery, CaimsDocument61 pagesShock: Dr. P. Manoj Kumar Asst. Professor, Dep. of Gen. Surgery, CaimsManoj Kumar PasunooriNo ratings yet
- Cardiac FailureDocument13 pagesCardiac FailureButool FatimaNo ratings yet
- Shock: Michael A. Puskarich Alan E. JonesDocument9 pagesShock: Michael A. Puskarich Alan E. JonesFarhanNo ratings yet
- SHOCK LEC Modified (2nd)Document86 pagesSHOCK LEC Modified (2nd)spanishthingz01No ratings yet
- Shock RosenDocument10 pagesShock RosenJuan GallegoNo ratings yet
- Shock: Rose Ann J. Raquiza-Perante Post Graduate InternDocument53 pagesShock: Rose Ann J. Raquiza-Perante Post Graduate InternRose Ann RaquizaNo ratings yet
- Shock Seminar-IDocument26 pagesShock Seminar-ISimran JosanNo ratings yet
- 04 ShockDocument142 pages04 ShockDefa3 madniNo ratings yet
- ShockDocument19 pagesShockirenekhatete1No ratings yet
- Stages of ShockDocument13 pagesStages of ShockA. P.No ratings yet
- Shock Shock: DR Budi Enoch SPPDDocument31 pagesShock Shock: DR Budi Enoch SPPDRoby KieranNo ratings yet
- 7 - Hemodynamic Disorders ShockDocument21 pages7 - Hemodynamic Disorders ShockShna SaadiNo ratings yet
- Dentistry L5 SHOCKDocument20 pagesDentistry L5 SHOCKHadeer WasfyNo ratings yet
- MR Elamin ShockDocument70 pagesMR Elamin ShockMohammed Abd AlgadirNo ratings yet
- Circulatory Shock: Dr. Niranjan Murthy H L Asst Prof of Physiology SSMC, TumkurDocument18 pagesCirculatory Shock: Dr. Niranjan Murthy H L Asst Prof of Physiology SSMC, TumkurnirilibNo ratings yet
- ShockDocument8 pagesShockАчпже Чпжечу100% (1)
- Circulatory Shock: Santosh DevDocument32 pagesCirculatory Shock: Santosh DevdevdsantoshNo ratings yet
- Types of Shock: Ms. Saheli Chakraborty 2 Year MSC Nursing Riner, BangaloreDocument36 pagesTypes of Shock: Ms. Saheli Chakraborty 2 Year MSC Nursing Riner, Bangaloremalathi100% (6)
- Notes On ShockDocument9 pagesNotes On ShockViswa GiriNo ratings yet
- TCHP Shock Series Part 2Document2 pagesTCHP Shock Series Part 2ikeernawatiNo ratings yet
- Shock - StatPearls - NCBI BookshelfDocument5 pagesShock - StatPearls - NCBI BookshelfSYAFIRA LAILA NURULITANo ratings yet
- Drug Used in The Therapy of Shock.Document8 pagesDrug Used in The Therapy of Shock.Vennela100% (1)
- SHOCKDocument35 pagesSHOCKsami azadNo ratings yet
- ShockDocument25 pagesShockAvneet Maan100% (1)
- Shock: Gastrointestinal Surgical Department of Affiliated Hospital of Jining Medical CollegeDocument52 pagesShock: Gastrointestinal Surgical Department of Affiliated Hospital of Jining Medical Collegesanjivdas100% (1)
- SHOCK LEC Modified (2nd)Document86 pagesSHOCK LEC Modified (2nd)spanishthingz01No ratings yet
- HMRG &shock 2022-2023Document54 pagesHMRG &shock 2022-2023Asraa ThjeelNo ratings yet
- Iadt03i5p345 PDFDocument15 pagesIadt03i5p345 PDFSudhit SethiNo ratings yet
- Shock Management: by Group 7Document87 pagesShock Management: by Group 7Nur Khairah AmalinaNo ratings yet
- Circulatory ShockDocument9 pagesCirculatory ShockTri UtomoNo ratings yet
- Diagnosis of Circulatory FailureDocument21 pagesDiagnosis of Circulatory FailureQuang Anh LeNo ratings yet
- Shock: Pathophysiology, Diagnosis, Treatment, and Physiologic Response To TraumaDocument12 pagesShock: Pathophysiology, Diagnosis, Treatment, and Physiologic Response To TraumaValentinaJiménezNo ratings yet
- ShockDocument36 pagesShockJohnryan NdiranguNo ratings yet
- In The Name of Allah, The Most Beneficent, The Most MercifulDocument40 pagesIn The Name of Allah, The Most Beneficent, The Most MercifulISMAILNo ratings yet
- Hypovolemic shock - A reviewDocument4 pagesHypovolemic shock - A reviewAmirullah AbdiNo ratings yet
- MEDICAL SURGICAL NURSING DISCUSSION ON SHOCKDocument22 pagesMEDICAL SURGICAL NURSING DISCUSSION ON SHOCKNavpreet Kaur100% (1)
- Manajemen Shock Dan PatofisologiDocument19 pagesManajemen Shock Dan PatofisologiRizki DunnirohNo ratings yet
- ShockDocument48 pagesShockanon-7341200% (2)
- Shock AssignmentDocument6 pagesShock Assignmentareebafarooq820No ratings yet
- Approach to Shock in 4 StagesDocument28 pagesApproach to Shock in 4 StagesSyasya ZulkiffliNo ratings yet
- Shock: Syahbuddin HarahapDocument41 pagesShock: Syahbuddin Harahapprima suci angrainiNo ratings yet
- Shock and BleedingDocument24 pagesShock and BleedingRaissa IcaNo ratings yet
- Seminar On Shock: IndexDocument37 pagesSeminar On Shock: IndexGayathri R100% (1)
- Shock: Ii PharmdDocument25 pagesShock: Ii PharmdBharath GowdaNo ratings yet
- Circulatory ShockDocument9 pagesCirculatory ShockVictor Euclides Briones MoralesNo ratings yet
- OPEN ACCESS TEXTBOOK OF GENERAL SURGERY: SEPTIC SHOCKDocument4 pagesOPEN ACCESS TEXTBOOK OF GENERAL SURGERY: SEPTIC SHOCKusamaNo ratings yet
- ShockDocument21 pagesShockMin-Joo Esther ParkNo ratings yet
- Br. J. Anaesth. 2012 Dutton I39 46Document8 pagesBr. J. Anaesth. 2012 Dutton I39 46fitrah fajrianiNo ratings yet
- Shock: Dr. Naser El-Hammuri Head of The Department of Surgery Hashemite UniversityDocument40 pagesShock: Dr. Naser El-Hammuri Head of The Department of Surgery Hashemite UniversityMohammad Husni BanisalmanNo ratings yet
- Circulatory Shock 18.12.2017Document11 pagesCirculatory Shock 18.12.2017Tamal MaityNo ratings yet
- 04 08 ShockDocument6 pages04 08 Shockthev0206No ratings yet
- Hypotension & ShockDocument22 pagesHypotension & ShockEkawati ErprismanNo ratings yet
- Untitled PresentationDocument11 pagesUntitled Presentationpectusexcavatum35No ratings yet
- Hemorrhagic ShockDocument29 pagesHemorrhagic ShockMusaNo ratings yet
- Definition, Causes, Types and Management of ShockDocument7 pagesDefinition, Causes, Types and Management of ShockShaker MUhammedNo ratings yet
- final SHOCK PPTDocument44 pagesfinal SHOCK PPTAbas AhmedNo ratings yet
- CirculatoryShock NejmraDocument9 pagesCirculatoryShock NejmraMaria Agostina EspecheNo ratings yet
- Central Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsFrom EverandCentral Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsNo ratings yet
- Assessment of bleeding Shock in a Politraumatized PatientFrom EverandAssessment of bleeding Shock in a Politraumatized PatientNo ratings yet
- Accountancy Vol 1 - EMDocument16 pagesAccountancy Vol 1 - EMGOWTHAM A 18MBA176No ratings yet
- CH 7 Blood Disorders F FF FDocument75 pagesCH 7 Blood Disorders F FF FZainab AbbasNo ratings yet
- Sales AssistantDocument1 pageSales AssistantZainab AbbasNo ratings yet
- Unilever Case Study: How Tim Allen Transformed the Struggling CompanyDocument6 pagesUnilever Case Study: How Tim Allen Transformed the Struggling CompanyZainab AbbasNo ratings yet
- Job Description for Sales Assistant RoleDocument2 pagesJob Description for Sales Assistant RoleZainab AbbasNo ratings yet
- Regional Data Centers - 2022 - v4Document1 pageRegional Data Centers - 2022 - v4Zainab AbbasNo ratings yet
- HR Report on Resolving Workplace ConflictsDocument3 pagesHR Report on Resolving Workplace ConflictsZainab AbbasNo ratings yet
- Thesis Lab BookDocument8 pagesThesis Lab Bookftinuckef100% (2)
- Chapter 06 - 192-217 PDFDocument26 pagesChapter 06 - 192-217 PDFMaria KolovouNo ratings yet
- SepsisScreenTreatmentAlgorithm BaylorUMedicalCenter PDFDocument66 pagesSepsisScreenTreatmentAlgorithm BaylorUMedicalCenter PDFFanie BeatriceNo ratings yet
- Lesson Plan On Shock and HaemorrhageDocument44 pagesLesson Plan On Shock and HaemorrhageVeenasravanthiNo ratings yet
- Surgery-I Review (2019)Document12 pagesSurgery-I Review (2019)Margaret ThatcherNo ratings yet
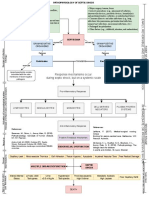
- Pathophysiology of Septic Shock Draft 1Document1 pagePathophysiology of Septic Shock Draft 1Ju Lie AnnNo ratings yet
- Literature Review On Knowledge Regarding Prevention of Cervical CancerDocument6 pagesLiterature Review On Knowledge Regarding Prevention of Cervical Cancerea8p6td0No ratings yet
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDocument15 pagesDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateHartanto SantosoNo ratings yet
- Clinical Management For Patients Admitted To A Critical Care Unit With Severe Sepsis or Septic ShockDocument7 pagesClinical Management For Patients Admitted To A Critical Care Unit With Severe Sepsis or Septic ShockrizkaNo ratings yet
- Critical Care NursingDocument85 pagesCritical Care NursinganreilegardeNo ratings yet
- Highlights - ACLS - LinearizedDocument34 pagesHighlights - ACLS - LinearizedRayssaNo ratings yet
- Test Taking StrategiesDocument85 pagesTest Taking StrategiesNyjil Patrick Basilio ColumbresNo ratings yet
- Understanding HemodynamicsDocument21 pagesUnderstanding HemodynamicsGiovanni Mictil86% (7)
- Syllabus For EMT BasicDocument51 pagesSyllabus For EMT BasicWevinneNo ratings yet
- Chapter 4 - Mixed Venous Oxygen SaturationDocument3 pagesChapter 4 - Mixed Venous Oxygen SaturationJamesNo ratings yet
- Fluid Management and Monitoring for Large BurnsDocument9 pagesFluid Management and Monitoring for Large BurnsEduardo Espin LanzNo ratings yet
- Sepsis en El Embarazo y PuerperioDocument9 pagesSepsis en El Embarazo y PuerperioJoseTeodomiroQuispeRicciNo ratings yet
- Unconscious Child AssessmentDocument52 pagesUnconscious Child Assessmentar bindraNo ratings yet
- 5 Management of Cardiogenic ShockDocument14 pages5 Management of Cardiogenic Shockileav_2No ratings yet
- Shock ManagementDocument26 pagesShock ManagementMuhammad Irfanuddin Bin IbrahimNo ratings yet
- Septic ShockDocument48 pagesSeptic ShockAnggie Drei IcuNo ratings yet
- Ch. 19. Postoperative Nursing CareDocument51 pagesCh. 19. Postoperative Nursing Careمحمد الحواجرةNo ratings yet
- Nursing Process and Midwifery AssessmentDocument20 pagesNursing Process and Midwifery AssessmentGreggy Francisco LaraNo ratings yet
- Intelligence Is Like A River: The Deeper It Is, The Less Noise It Makes.Document88 pagesIntelligence Is Like A River: The Deeper It Is, The Less Noise It Makes.reccelle_pre295747No ratings yet
- TOPNOTCH MEDICAL BOARD PREP IM GUAZON CASEDocument6 pagesTOPNOTCH MEDICAL BOARD PREP IM GUAZON CASEJey Gee DeeNo ratings yet
- SirsDocument29 pagesSirsfatimaNo ratings yet
- EFA - Module 2 r1Document57 pagesEFA - Module 2 r1Jerry CañeroNo ratings yet
- Burn InjuryDocument32 pagesBurn InjuryamosNo ratings yet
- Effects of Vasopressin in Septic Shock: Case StudyDocument7 pagesEffects of Vasopressin in Septic Shock: Case Studyns_karaniaNo ratings yet
- Perioperative Nursing Care OverviewDocument216 pagesPerioperative Nursing Care Overviewmaricor_28174462No ratings yet