You might also like
- Hip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDocument38 pagesHip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDr'Dinesh MishraNo ratings yet
- HIp & Knee Extremity Notes Sorgenfrey Gindl 7.16.10Document116 pagesHIp & Knee Extremity Notes Sorgenfrey Gindl 7.16.10joe joeNo ratings yet
- Cat 2Document5 pagesCat 2Edgardo BivimasNo ratings yet
- Perspectives From Parents of Children With and Without ExceptionalitiesDocument103 pagesPerspectives From Parents of Children With and Without ExceptionalitiesFranNo ratings yet
- Reinold - Glenohumeral and Scapulothoracic RehabDocument45 pagesReinold - Glenohumeral and Scapulothoracic Rehabshivnair100% (2)
- The Wrist Common Injuries and ManagementDocument36 pagesThe Wrist Common Injuries and ManagementDan RollorataNo ratings yet
- Postural DeviationsDocument40 pagesPostural DeviationsMohamed Tariq Acchha100% (2)
- 2 Biomechanics of The ShoulderDocument47 pages2 Biomechanics of The ShoulderDaniel PereiraNo ratings yet
- GAIT 2 - Clinical Gait Analysis - HandoutDocument32 pagesGAIT 2 - Clinical Gait Analysis - Handoutj100% (1)
- Orthopedic: Dislocations of The Hip JointDocument16 pagesOrthopedic: Dislocations of The Hip JointAnmarNo ratings yet
- Joint Mobilization What Is Joint Mobilization?Document6 pagesJoint Mobilization What Is Joint Mobilization?taravindnagarajNo ratings yet
- Hip Labral Repair PresentationDocument15 pagesHip Labral Repair Presentationapi-612728940No ratings yet
- 9 Hip & Lumber DDDocument29 pages9 Hip & Lumber DDHeba Abo bakrNo ratings yet
- Hip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentFrom EverandHip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentNo ratings yet
- Hip & Groin Pain DD PDFDocument15 pagesHip & Groin Pain DD PDFagniosaiNo ratings yet
- Conservative Treatment For Meniscus RehabilitationDocument2 pagesConservative Treatment For Meniscus RehabilitationShahroz Khan100% (1)
- Spine Biomechanics: Mer/Bio Soft Tissue Mechanics SB-1Document11 pagesSpine Biomechanics: Mer/Bio Soft Tissue Mechanics SB-1Sarah Magdy100% (1)
- Flexor Tendon Injuries SeminarDocument75 pagesFlexor Tendon Injuries SeminarAmit GoyalNo ratings yet
- Marriott Consumer Incentives Overview: Who We AreDocument46 pagesMarriott Consumer Incentives Overview: Who We AreAshleyFurnitureNo ratings yet
- NexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29Document48 pagesNexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29flo1987No ratings yet
- Typical Shoulder TroublesDocument7 pagesTypical Shoulder TroublesLev KalikaNo ratings yet
- The Foot Posture Index: Six Item Version FPI-6 User Guide and ManualDocument19 pagesThe Foot Posture Index: Six Item Version FPI-6 User Guide and ManualBryan AlimNo ratings yet
- Achilles RuptureDocument23 pagesAchilles RupturePhysiotherapist AliNo ratings yet
- Hamstring Injuries A Discussion of Physiotherapy RehabDocument24 pagesHamstring Injuries A Discussion of Physiotherapy RehabdracoscribdNo ratings yet
- Tendon Problems in Athletic IndividualsDocument15 pagesTendon Problems in Athletic IndividualsMuhammadskNo ratings yet
- IvdpDocument89 pagesIvdpFelix SabuNo ratings yet
- Distance Between WeldsDocument2 pagesDistance Between Weldshendraox3996100% (1)
- Basic Principles of Tendon TransferDocument10 pagesBasic Principles of Tendon TransferyeapdshengNo ratings yet
- Lumbar Spine AssessmentDocument26 pagesLumbar Spine Assessmentyoyo_pt2007100% (1)
- HIP JOINT Special Tests-WPS OfficeDocument51 pagesHIP JOINT Special Tests-WPS OfficeManisha Mishra100% (1)
- Soft Tissue Balance KneeDocument10 pagesSoft Tissue Balance KneeNitin BansalNo ratings yet
- InvoiceDocument1 pageInvoicesonu baliyanNo ratings yet
- Tennis Elbow or Lateral Epicondylitis: Key PointsDocument10 pagesTennis Elbow or Lateral Epicondylitis: Key PointsMarliani AfriastutiNo ratings yet
- Famous People With Mental Illness Powerpoint PresentationDocument36 pagesFamous People With Mental Illness Powerpoint Presentationzakir aliNo ratings yet
- Alingment in TKRDocument3 pagesAlingment in TKRdeepak100% (1)
- A Regional Approach To Foot and Ankle MRIDocument17 pagesA Regional Approach To Foot and Ankle MRInior100% (1)
- PostureDocument2 pagesPostureNader MorrisNo ratings yet
- Scapular DyskinesisDocument24 pagesScapular DyskinesisbarbaraNo ratings yet
- Total Knee Replacement: The Path ToDocument6 pagesTotal Knee Replacement: The Path ToMoses DhinakarNo ratings yet
- Y-DNA Haplogroup GDocument9 pagesY-DNA Haplogroup GcgonzagaaNo ratings yet
- Seiichi Ishibashi (Auth.) - Dictionary of Electronics and Electrical Engineering - English-Japanese-German-Russian-Springer US (1995) PDFDocument1,801 pagesSeiichi Ishibashi (Auth.) - Dictionary of Electronics and Electrical Engineering - English-Japanese-German-Russian-Springer US (1995) PDFCarlos Licea100% (1)
- Shoulder Arthroscopy Presentation v0.4Document20 pagesShoulder Arthroscopy Presentation v0.4Mohammad Nasfikur Rahman KhanNo ratings yet
- Patellofemoral InstabilityDocument10 pagesPatellofemoral InstabilitysionforjanNo ratings yet
- Clinical Signs - NamedDocument9 pagesClinical Signs - NamedsprapurNo ratings yet
- Pediatric Foot DeformitiesDocument27 pagesPediatric Foot DeformitieszeshmaNo ratings yet
- Sport Injuries: ShoulderDocument67 pagesSport Injuries: ShoulderNabiha AjmalNo ratings yet
- Neck PainDocument1 pageNeck PainHasan RahmanNo ratings yet
- Hip Knee Ankle Foot OrthosisDocument44 pagesHip Knee Ankle Foot OrthosisGulzar Ahmad100% (1)
- Ankel Heel PainDocument51 pagesAnkel Heel PainMeno Ali100% (1)
- Foot and Ankle KinesiologDocument95 pagesFoot and Ankle KinesiologCristine RamosNo ratings yet
- KAFODocument34 pagesKAFOBedo GikryNo ratings yet
- Pressure Measurement in The Gait LabDocument22 pagesPressure Measurement in The Gait LabdariandNo ratings yet
- Three-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerDocument34 pagesThree-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerMuhammad Safwan Ahmad FadzilNo ratings yet
- DR Ashwani Panchal Jss Medical College MysoreDocument94 pagesDR Ashwani Panchal Jss Medical College MysoreAravind RvndNo ratings yet
- Numerical SimulationsDocument530 pagesNumerical SimulationsRemus Costan100% (1)
- Gpe - 017.1 - Orthopaedic ExaminationDocument3 pagesGpe - 017.1 - Orthopaedic ExaminationImiey Eleena HanumNo ratings yet
- Dynamic Stability of Thin-Walled Structures: A Semi-AnalyticalDocument244 pagesDynamic Stability of Thin-Walled Structures: A Semi-Analyticalnjm00175% (4)
- Epp, It's All About VariantsDocument35 pagesEpp, It's All About VariantsMichkasegat100% (2)
- Internal Control - Hayes - Chapter 6Document44 pagesInternal Control - Hayes - Chapter 6saif khanNo ratings yet
- Gait and Gait Aids-Muscle WeeknessDocument57 pagesGait and Gait Aids-Muscle WeeknessKurniawanFirstNo ratings yet
- Distal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiDocument5 pagesDistal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiPhysiotherapy Care SpecialistsNo ratings yet
- Distal Femur (Sandeep Sir)Document22 pagesDistal Femur (Sandeep Sir)Kirubakaran Saraswathy PattabiramanNo ratings yet
- Joint Mobilizations PDFDocument1 pageJoint Mobilizations PDFErik TellezNo ratings yet
- Approach To FractureDocument17 pagesApproach To FractureRebecca WongNo ratings yet
- Orthopaedic Instruments and ImplantsDocument21 pagesOrthopaedic Instruments and ImplantsgibreilNo ratings yet
- Special Test KNEE UnaDocument25 pagesSpecial Test KNEE Unasingle_ladyNo ratings yet
- 2018 Hip Program FINALDocument119 pages2018 Hip Program FINALJafild Fild riverNo ratings yet
- Tennis ElbowDocument13 pagesTennis ElbowPadma PadalNo ratings yet
- Tennis Elbow JOSPT ArticleDocument11 pagesTennis Elbow JOSPT ArticleHasan RahmanNo ratings yet
- Kibler Et Al 2012 Scapula Dyskinesis and Its Relation To Shoulder Injury PDFDocument9 pagesKibler Et Al 2012 Scapula Dyskinesis and Its Relation To Shoulder Injury PDFPamela DíazNo ratings yet
- Hospitality Supervision and Training SkillsDocument11 pagesHospitality Supervision and Training SkillsPunam Garu100% (2)
- The Basic Economic Order Quantity ModelDocument13 pagesThe Basic Economic Order Quantity ModelRichardson HolderNo ratings yet
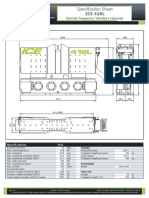
- Specification Sheet: ICE 416LDocument2 pagesSpecification Sheet: ICE 416LBapusaheb GuthaleNo ratings yet
- Civic Education G10 NotesDocument39 pagesCivic Education G10 NotesMasitala PhiriNo ratings yet
- AI (ACO) - ANT Colony OptimizationDocument2 pagesAI (ACO) - ANT Colony OptimizationRoop GoswamiNo ratings yet
- Tugas 2 Bahasa Inggris - Michelle Angel TanjungDocument3 pagesTugas 2 Bahasa Inggris - Michelle Angel TanjungNALLO BROONo ratings yet
- Boost Plan For Bnak Job by Latifur's Focus WritingDocument8 pagesBoost Plan For Bnak Job by Latifur's Focus WritingMonjurul Islam NafisNo ratings yet
- DR B R Ambedkar and Making of The Constitution A Case Study of Indian FederalismDocument13 pagesDR B R Ambedkar and Making of The Constitution A Case Study of Indian FederalismDanexNo ratings yet
- 7A Vocabulary - Test of Mini-Lessons 3.4, 3.5 & 3.6 Match The Words in The Table Below To Their Meanings As in The ExampleDocument4 pages7A Vocabulary - Test of Mini-Lessons 3.4, 3.5 & 3.6 Match The Words in The Table Below To Their Meanings As in The ExampleHussam Dawood Al-AreeqiNo ratings yet
- Overview of Literary Periods and MovementsDocument92 pagesOverview of Literary Periods and MovementsZarah Joyce SegoviaNo ratings yet
- Abstinence Journal ReflectionDocument3 pagesAbstinence Journal Reflectionapi-451295416No ratings yet
- FinalPrelimShort-Quiz (Rovelyn C. Lamor)Document3 pagesFinalPrelimShort-Quiz (Rovelyn C. Lamor)RO VENo ratings yet
- DAY 1 Passage 1Document2 pagesDAY 1 Passage 1wick90715No ratings yet
- Love SongDocument5 pagesLove SongTom N JerryNo ratings yet
- DISS 6thDocument31 pagesDISS 6thjoelNo ratings yet
- Nitrofurantoin 50 and 100 MF UKPARDocument30 pagesNitrofurantoin 50 and 100 MF UKPARdivyenshah3No ratings yet
- Basic CommandsDocument10 pagesBasic Commandssamsul rosadiNo ratings yet
- Grade 11 2nd Parallel Assessment SampleDocument3 pagesGrade 11 2nd Parallel Assessment SampleElaiza Tautho100% (1)