You might also like
- Haemopoiesis: Composition of Whole Blood & Its ComponentsDocument8 pagesHaemopoiesis: Composition of Whole Blood & Its ComponentsSafiya JamesNo ratings yet
- Chapter 17 Anatomy and Physiology NotesDocument10 pagesChapter 17 Anatomy and Physiology NotesZachary WatsonNo ratings yet
- Blood Cells and The Hematopoetic SystemDocument53 pagesBlood Cells and The Hematopoetic SystemMeet RandhawaNo ratings yet
- Hematology - A - RBCsDocument27 pagesHematology - A - RBCsAhmed Hassan KabarNo ratings yet
- Blood Physiology: Understanding Hemopoiesis and Anemia DiagnosisDocument23 pagesBlood Physiology: Understanding Hemopoiesis and Anemia DiagnosisOmar MaanNo ratings yet
- Chapter 19 - BloodDocument5 pagesChapter 19 - Bloodtomorrow.today.yesterday .yesterdayNo ratings yet
- Blood Composition and FunctionsDocument11 pagesBlood Composition and Functionsshapan biswaNo ratings yet
- Red Blood Cells, Anemia, and PolycythemiaDocument7 pagesRed Blood Cells, Anemia, and PolycythemiaShi no Me100% (1)
- Blood Lectie Generala Eng-2454Document56 pagesBlood Lectie Generala Eng-2454IngaŞaragovNo ratings yet
- BLG111Document7 pagesBLG111Manasseh LawrenceNo ratings yet
- Topic 29: Pathophysiology of Red Cell Series: 1. HematopoiesisDocument10 pagesTopic 29: Pathophysiology of Red Cell Series: 1. HematopoiesisAelita RuseelNo ratings yet
- Blood HBDocument31 pagesBlood HBBHUWAN BASKOTANo ratings yet
- Lec-1 Hematopoiesis and RBCsDocument38 pagesLec-1 Hematopoiesis and RBCsMuna MNo ratings yet
- Hematopoietic System OverviewDocument66 pagesHematopoietic System OverviewVerla MfeerNo ratings yet
- General Function of The BloodDocument25 pagesGeneral Function of The BloodMsKizzyNo ratings yet
- BLOOD PresentationDocument33 pagesBLOOD PresentationLezlie Jane SahaliNo ratings yet
- Blood Disorders 11Document50 pagesBlood Disorders 11Purnendu ParidaNo ratings yet
- Introduction To HematologyDocument95 pagesIntroduction To HematologyAhmad Farhan Hassan0% (1)
- Physiology Lec 1Document6 pagesPhysiology Lec 1Hussein AlaNo ratings yet
- Review of Red Blood Cells (Erythrocytes) and Hemolytic AnemiaDocument7 pagesReview of Red Blood Cells (Erythrocytes) and Hemolytic AnemiaStanley AnadiNo ratings yet
- Blood physiology components and functionsDocument39 pagesBlood physiology components and functionsSarmad Laith MortadaNo ratings yet
- BLOOD Update-1Document56 pagesBLOOD Update-1ahmadfadi343No ratings yet
- Physio. D. Suroor. L1. BloodDocument24 pagesPhysio. D. Suroor. L1. Bloodزين العابدين محمد عويشNo ratings yet
- Hematology 2020Document63 pagesHematology 2020odiodi57No ratings yet
- Physiology of Blood: Ratna Kusumawati Department of Physiology, Faculty of Medicine Universitas Sebelas Maret SurakartaDocument60 pagesPhysiology of Blood: Ratna Kusumawati Department of Physiology, Faculty of Medicine Universitas Sebelas Maret SurakartaZidaneNo ratings yet
- Blood: - Enzymes, E.G. Certain Clotting FactorsDocument14 pagesBlood: - Enzymes, E.G. Certain Clotting FactorsDerrick kinyaNo ratings yet
- Composition and Functions: BloodDocument86 pagesComposition and Functions: BloodYeyeh SantosNo ratings yet
- BloodDocument13 pagesBloodمحمد احمدNo ratings yet
- Chapter 32 Assessment of Hematologic Function and Treatment ModalitiesDocument19 pagesChapter 32 Assessment of Hematologic Function and Treatment ModalitiesAira Anne Tonee Villamin100% (3)
- Characteristics and Functions of Blood ComponentsDocument51 pagesCharacteristics and Functions of Blood ComponentssamayaNo ratings yet
- Physiology Clinical NotesDocument10 pagesPhysiology Clinical NotesMohammed EljackNo ratings yet
- Anemia 1Document104 pagesAnemia 1maryam ijazNo ratings yet
- Blood and Lymph [Autosaved]Document46 pagesBlood and Lymph [Autosaved]Shaikh SaqibNo ratings yet
- Blood cells, coagulation overviewDocument7 pagesBlood cells, coagulation overviewsenjicsNo ratings yet
- 1 HemopoiesisDocument30 pages1 Hemopoiesiscefolob289No ratings yet
- Aplastic AnemiaDocument7 pagesAplastic Anemianeil052288% (8)
- The Circulatory System:: BloodDocument101 pagesThe Circulatory System:: BloodAntonio MihaiNo ratings yet
- Blood CirculatoryDocument5 pagesBlood CirculatoryRekesh SaeedNo ratings yet
- Physiology of Blood: Ratna Kusumawati Department of Physiology, Faculty of Medicine Universitas Sebelas Maret SurakartaDocument65 pagesPhysiology of Blood: Ratna Kusumawati Department of Physiology, Faculty of Medicine Universitas Sebelas Maret SurakartaRizal AbdurrahmanNo ratings yet
- 2 CVS BloodDocument26 pages2 CVS BloodSepo CaciousNo ratings yet
- Chapter 17 Blood and 18 Review AnswersDocument4 pagesChapter 17 Blood and 18 Review Answersmamun0zNo ratings yet
- RBC Formation, Types of Anemia & Hemoglobin FunctionDocument2 pagesRBC Formation, Types of Anemia & Hemoglobin FunctionSittie Salma RegaroNo ratings yet
- Functions and Properties of Blood - Plasma - Blood Cell Production - Erythrocytes - Blood Types - Leukocytes - Hemostasis (Stoppage of Bleeding)Document47 pagesFunctions and Properties of Blood - Plasma - Blood Cell Production - Erythrocytes - Blood Types - Leukocytes - Hemostasis (Stoppage of Bleeding)vanderphysNo ratings yet
- Blood Formation& RBC 17TH AUGDocument19 pagesBlood Formation& RBC 17TH AUGNitin AroraNo ratings yet
- Unit 3 - BloodDocument51 pagesUnit 3 - BloodzulieyanaNo ratings yet
- The Significance of Blood: A Concise Look at its Composition and FunctionsDocument10 pagesThe Significance of Blood: A Concise Look at its Composition and FunctionsMaqbul AlamNo ratings yet
- Chapter 4 Blood Coagulation and Coagulation Disorders _32f6d4d0c67589df3863ad91f445f357Document27 pagesChapter 4 Blood Coagulation and Coagulation Disorders _32f6d4d0c67589df3863ad91f445f357daisysintszwaiNo ratings yet
- Blood Lectures 2014 PIO 205Document84 pagesBlood Lectures 2014 PIO 205Philip Abayomi VincentNo ratings yet
- Blood 2022Document49 pagesBlood 2022Fady FadyNo ratings yet
- Blood BiochemistryDocument124 pagesBlood BiochemistrySohail AhamdNo ratings yet
- Blood ReviewDocument13 pagesBlood ReviewDeleted AccountNo ratings yet
- WEEK 5 RBCS PPT AshDocument73 pagesWEEK 5 RBCS PPT AshotaibynaifNo ratings yet
- Histology & Cell BiologyDocument33 pagesHistology & Cell BiologyMohSen100% (1)
- Anatomi Fisiologi Manusia: HematologiDocument54 pagesAnatomi Fisiologi Manusia: HematologiARUMNo ratings yet
- Blood: MR Marudhar Associate Professor Nims UniversityDocument67 pagesBlood: MR Marudhar Associate Professor Nims UniversityDr-Marudhar MarudharNo ratings yet
- Hematologic SystemDocument81 pagesHematologic Systemseigelystic100% (23)
- Cardiovascular System: BloodDocument5 pagesCardiovascular System: BloodKoh Yen SinNo ratings yet
- Types Of Hemolytic Anemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandTypes Of Hemolytic Anemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- The Dental Plaque Biofilm MatrixDocument25 pagesThe Dental Plaque Biofilm MatrixTasha FarahNo ratings yet
- SGFP Common Fee Codes 09 6REVDocument4 pagesSGFP Common Fee Codes 09 6REVeschiuNo ratings yet
- OGUK Medical FormDocument7 pagesOGUK Medical Formum erNo ratings yet
- DRUG DOSAGE INDICATION CONTRAINDICATIONDocument2 pagesDRUG DOSAGE INDICATION CONTRAINDICATIONEurielle MioleNo ratings yet
- Tiket Juragan GombalDocument3 pagesTiket Juragan Gombaldhebys suryaniNo ratings yet
- Chemistry Project RoughDocument16 pagesChemistry Project RoughDinakaran JaganNo ratings yet
- Prevalence of Diabetes, Associated Symptoms and Risk Factors Among University StudentsDocument8 pagesPrevalence of Diabetes, Associated Symptoms and Risk Factors Among University Studentsijmb333No ratings yet
- Medicine: The Effectiveness of Tai Chi For Postpartum DepressionDocument4 pagesMedicine: The Effectiveness of Tai Chi For Postpartum DepressionNisa RohmatinNo ratings yet
- Med-Surg Exam #2 Study GuideDocument33 pagesMed-Surg Exam #2 Study GuideCaitlyn BilbaoNo ratings yet
- Soal Compile Hemato-OncologyDocument25 pagesSoal Compile Hemato-OncologyDapot SianiparNo ratings yet
- PROBLEM PRIORITY SETTING (Acob)Document3 pagesPROBLEM PRIORITY SETTING (Acob)Audrey Ann AcobNo ratings yet
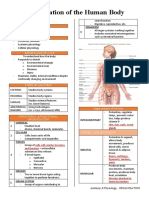
- Organization of the Human BodyDocument8 pagesOrganization of the Human BodyAly HannahNo ratings yet
- NCP (Fatigue)Document1 pageNCP (Fatigue)student_019100% (1)
- Mechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeDocument12 pagesMechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeGayathri RNo ratings yet
- Urinary SystemDocument9 pagesUrinary SystemMary Joyce RamosNo ratings yet
- Bio Project 2-3Document7 pagesBio Project 2-3ISHWARYANo ratings yet
- Infectii Oportuniste CovidDocument12 pagesInfectii Oportuniste CovidAndreea CiorneaNo ratings yet
- Neurologic ExaminationDocument67 pagesNeurologic Examinationሀይደር ዶ.ር100% (1)
- A008 MicroVue C4d EnglishDocument15 pagesA008 MicroVue C4d EnglishAlisNo ratings yet
- Psychi BulletDocument4 pagesPsychi BulletHEALTH TIPSNo ratings yet
- Case StudyDocument2 pagesCase StudyClaire MachicaNo ratings yet
- Chapter 3 - The Polygraph TechniqueDocument16 pagesChapter 3 - The Polygraph Techniqueキャロル アンNo ratings yet
- Daily Lesson Plan in English Grade 7 (Quarter 3-Module 5)Document2 pagesDaily Lesson Plan in English Grade 7 (Quarter 3-Module 5)Ramil60% (5)
- Automated Detection of Diabetic Foot With and Without Neuropathy Using Double Density-Dual Tree-Complex Wavelet Transform On Foot ThermogramsDocument32 pagesAutomated Detection of Diabetic Foot With and Without Neuropathy Using Double Density-Dual Tree-Complex Wavelet Transform On Foot ThermogramsLuis Martínez RamírezNo ratings yet
- 3.5 PHARMA ANTI MYCOBACTERIAL AGENTSpdfDocument18 pages3.5 PHARMA ANTI MYCOBACTERIAL AGENTSpdfJanet SantosNo ratings yet
- Chest PhysiotherapyDocument4 pagesChest Physiotherapyhakky gamyNo ratings yet
- Antibacterial Activity of Thaaleesaadhi Chooranam Against Human PathogensDocument8 pagesAntibacterial Activity of Thaaleesaadhi Chooranam Against Human PathogensRAJ KUMARNo ratings yet
- Absorb Amplify Course List (Updated Monthly)Document6 pagesAbsorb Amplify Course List (Updated Monthly)Madhu KumarNo ratings yet
- Kisi 2 B Ing - 230604 - 173816Document3 pagesKisi 2 B Ing - 230604 - 173816izzatul afifahNo ratings yet
- Review of Trichomonas Vaginalisinfection From (2013-2023) in Governorates of IraqDocument8 pagesReview of Trichomonas Vaginalisinfection From (2013-2023) in Governorates of IraqIJAR JOURNALNo ratings yet
































![Blood and Lymph [Autosaved]](https://imgv2-2-f.scribdassets.com/img/document/724029416/149x198/d1a5a33b7c/1713378683?v=1)