You might also like
- Platelet Protocols: Research and Clinical Laboratory ProceduresFrom EverandPlatelet Protocols: Research and Clinical Laboratory ProceduresNo ratings yet
- Introduction To HemostasisDocument45 pagesIntroduction To Hemostasismedino100% (3)
- Blood Coagulation: Presenter: DR Pashi V Moderator: DR Zulu RDocument53 pagesBlood Coagulation: Presenter: DR Pashi V Moderator: DR Zulu RRabia AhmadNo ratings yet
- PlateletsDocument35 pagesPlateletsSiĦãm Mỡ100% (1)
- HemostasisDocument21 pagesHemostasisilyasNo ratings yet
- Hemostasis and Blood CoagulationDocument35 pagesHemostasis and Blood CoagulationHarun MohamedNo ratings yet
- Haemostasis: DR Sri Lestari Sulistyo Rini, MSCDocument56 pagesHaemostasis: DR Sri Lestari Sulistyo Rini, MSCelfianaNo ratings yet
- Platelets. Hemostasis.: Learning ObjectivesDocument37 pagesPlatelets. Hemostasis.: Learning ObjectivesQasim alaliNo ratings yet
- Bleeding Disorders 1Document152 pagesBleeding Disorders 1Shameena KnNo ratings yet
- PHS 221 HaemostasisDocument36 pagesPHS 221 Haemostasismetasynthronos748No ratings yet
- Hemostasis: Presenter-Dr. SonuDocument68 pagesHemostasis: Presenter-Dr. SonukiranNo ratings yet
- Haematology Lecture 7+8Document34 pagesHaematology Lecture 7+8Nabeel TahirNo ratings yet
- Haemostasis: Case StudyDocument19 pagesHaemostasis: Case StudyTusabe FredNo ratings yet
- Arterial Thrombosis and EmbolismDocument43 pagesArterial Thrombosis and EmbolismA A D H INo ratings yet
- Lecture 6 - BloodDocument5 pagesLecture 6 - Bloodadnan yaqoobNo ratings yet
- Unit IV HemostasisDocument49 pagesUnit IV Hemostasisalshads957No ratings yet
- Lecture 4-HemostasisDocument34 pagesLecture 4-HemostasissamayaNo ratings yet
- Haemostasis Foundation 1-October 2010Document51 pagesHaemostasis Foundation 1-October 2010cute_sakura_03No ratings yet
- Components of The HaemostaticDocument25 pagesComponents of The HaemostaticRo RyNo ratings yet
- Farmakoterapi Coagulation DisorderDocument55 pagesFarmakoterapi Coagulation DisorderNur Astuty PurnamasariNo ratings yet
- Platelets-Composition, Function, Hemostasis and Its Individual PhasesDocument14 pagesPlatelets-Composition, Function, Hemostasis and Its Individual PhasesHebsiba PonnayyanNo ratings yet
- 01 Pathophysiology of Cardiovascular Diseases THOMBOSISDocument27 pages01 Pathophysiology of Cardiovascular Diseases THOMBOSISdona donneNo ratings yet
- PlateletsDocument23 pagesPlateletsnirilibNo ratings yet
- Approach To Bleeding NeonateDocument20 pagesApproach To Bleeding NeonateIndranil DuttaNo ratings yet
- 1.02 Hemostasis and CoagulationDocument4 pages1.02 Hemostasis and CoagulationShiena ArchividoNo ratings yet
- Aula Af 2 PDFDocument49 pagesAula Af 2 PDFtobiasmanuel179No ratings yet
- Hematology Unit: Dr. Furqan HashmiDocument32 pagesHematology Unit: Dr. Furqan HashmiabubakarNo ratings yet
- Platelets (Or) Thrombocytes BY U.Sivakumar: 1 PhysiologyDocument40 pagesPlatelets (Or) Thrombocytes BY U.Sivakumar: 1 PhysiologyAkash JaatNo ratings yet
- Bleeding Clotting Disorders I FREEMAN 20131Document90 pagesBleeding Clotting Disorders I FREEMAN 20131Elleason Joshua G. FranciscoNo ratings yet
- Haemostasis: Dr. Ali ElhassanDocument45 pagesHaemostasis: Dr. Ali ElhassanMohja JaberNo ratings yet
- 11-Components of The Haemostatic ResponseDocument45 pages11-Components of The Haemostatic ResponseNipun ShamikaNo ratings yet
- Anticoagulants, Fibrinolytics, AntiplateletsDocument88 pagesAnticoagulants, Fibrinolytics, Antiplateletspmuawiyah25No ratings yet
- مستند PDF-3C57C64C1675-1Document15 pagesمستند PDF-3C57C64C1675-1lorenoh21No ratings yet
- Seminar 4th WeekDocument33 pagesSeminar 4th WeekBibo BobiNo ratings yet
- 11 Coagulation PDFDocument51 pages11 Coagulation PDFمحمد علي حريج / مسائيNo ratings yet
- DR Madzlifah AhadonDocument98 pagesDR Madzlifah AhadonFrances Lau Yee ChinNo ratings yet
- He Most As IsDocument22 pagesHe Most As IsFiras Nazih Bou DiabNo ratings yet
- Blood Mbbs 11 25 Jan 23Document35 pagesBlood Mbbs 11 25 Jan 23GITANSHU GALGATNo ratings yet
- Hema Prelim MergedDocument112 pagesHema Prelim MergedRich Darlene Dela CruzNo ratings yet
- Platelet Function Tests - DR Makboul 2018 PDFDocument50 pagesPlatelet Function Tests - DR Makboul 2018 PDFmagendi indra muktiNo ratings yet
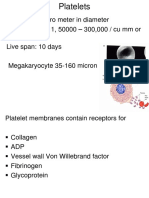
- Size: 1 - 4 Micro Meter in Diameter Normal Count: 1, 50000 - 300,000 / Cu MM or Micro Liter Live Span: 10 DaysDocument9 pagesSize: 1 - 4 Micro Meter in Diameter Normal Count: 1, 50000 - 300,000 / Cu MM or Micro Liter Live Span: 10 DaysFauzan AdzNo ratings yet
- PlateletsDocument94 pagesPlateletsShraddha PatilNo ratings yet
- Hemostasis, Hemorrhagic Disorders and ThrombosisDocument114 pagesHemostasis, Hemorrhagic Disorders and ThrombosisZeeNo ratings yet
- Coagulation CascadeDocument41 pagesCoagulation CascadeJae TNo ratings yet
- Hemostasis, Clotting, EctDocument33 pagesHemostasis, Clotting, Ectblessing akataNo ratings yet
- HRM Week 2 - Introduction 2020 - PrintDocument34 pagesHRM Week 2 - Introduction 2020 - PrintShiv SookunNo ratings yet
- Blood Physiology: Dr. Meg-Angela Christi AmoresDocument29 pagesBlood Physiology: Dr. Meg-Angela Christi AmoresSara SabraNo ratings yet
- 1-2 Hemostasis PhysiologyDocument48 pages1-2 Hemostasis PhysiologyHussein Al Saedi100% (2)
- Hemostasis: Vasoconstriction Platelet Plug Formation Coagulation Cascade FibrinolysisDocument17 pagesHemostasis: Vasoconstriction Platelet Plug Formation Coagulation Cascade FibrinolysisRawat GamingNo ratings yet
- Normal Hemostasis: Tutor 2Document21 pagesNormal Hemostasis: Tutor 2Salsabilla Ameranti PutriNo ratings yet
- PLATELETES Mls and NursingDocument12 pagesPLATELETES Mls and NursingTimothy usmanNo ratings yet
- Bleeding Disorders - DR RashaDocument95 pagesBleeding Disorders - DR RashaRasha TelebNo ratings yet
- Blood Coagulation SeminarDocument115 pagesBlood Coagulation SeminarmeghaNo ratings yet
- Cardiovascular PDFDocument41 pagesCardiovascular PDFBrian Aldous FernandezNo ratings yet
- Introduction To Blood CoagulationDocument22 pagesIntroduction To Blood Coagulationemman_abzNo ratings yet
- Module 1 - Blood Vasculature, Megakaryocytes and PlateletsDocument31 pagesModule 1 - Blood Vasculature, Megakaryocytes and PlateletsI love dem Coffee (Migz)No ratings yet
- Physiology of CoagulationDocument16 pagesPhysiology of CoagulationIlyas HalimNo ratings yet
- Primary Haemostatic Disorders: DR C AlexisDocument73 pagesPrimary Haemostatic Disorders: DR C AlexisRonaldoNo ratings yet
- Blood Cells and CoagulationDocument26 pagesBlood Cells and CoagulationHoàngBảoLongNo ratings yet
- Hemophilia in ChildrenDocument6 pagesHemophilia in Childrensimina intunericNo ratings yet
- HemophiliaDocument3 pagesHemophiliasanghamitra jana0% (1)
- Properties of The Plasma ProcoagulantsDocument4 pagesProperties of The Plasma ProcoagulantsBabylene MamauagNo ratings yet
- Vitamin K TOFDocument5 pagesVitamin K TOFNanank Akhiruddin SyamsaNo ratings yet
- Edema: USMLE Step 1 Web Prep - Circulatory PathologyDocument9 pagesEdema: USMLE Step 1 Web Prep - Circulatory PathologyfrabziNo ratings yet
- Review Article: The Role of Thrombophilia in PregnancyDocument14 pagesReview Article: The Role of Thrombophilia in PregnancyTina GrosuNo ratings yet
- 5 Bleeding Disorders PPT EditedDocument87 pages5 Bleeding Disorders PPT EditedFrances Isabella OlasimanNo ratings yet
- Haematinics, Coagulants and Anticoagulant - DR - Jibachha Sah, M.V.SC, LecturerDocument27 pagesHaematinics, Coagulants and Anticoagulant - DR - Jibachha Sah, M.V.SC, Lecturerjibachha sahNo ratings yet
- Hema 2 5th Ed SummaryDocument9 pagesHema 2 5th Ed Summarymonzon.mika1801No ratings yet
- TT Test LabDocument2 pagesTT Test LabSamantha ReynoldsNo ratings yet
- DapusDocument4 pagesDapusRuth VeraulinaNo ratings yet
- Haemostasis and Thrombosis: An Overview: H. RascheDocument5 pagesHaemostasis and Thrombosis: An Overview: H. Rascheshinichi kudoNo ratings yet
- Alyana Ellaine S. Matias, MDDocument24 pagesAlyana Ellaine S. Matias, MDAlyana MatiasNo ratings yet
- Farmakoterapi Coagulation DisorderDocument55 pagesFarmakoterapi Coagulation DisorderNur Astuty PurnamasariNo ratings yet
- MCQ ON Acute Posthemorrhagic AnemiaDocument22 pagesMCQ ON Acute Posthemorrhagic AnemiaSampath KumarNo ratings yet
- Laboratory Evaluation of PlateletsDocument4 pagesLaboratory Evaluation of Plateletscherry nokiaNo ratings yet
- Morning Report IBS 17 Oktober 2017 DR Tendi Novara, Sp. AnDocument13 pagesMorning Report IBS 17 Oktober 2017 DR Tendi Novara, Sp. AnLathif SuryandanaNo ratings yet
- Combined HemaDocument28 pagesCombined HemaViena Mae MaglupayNo ratings yet
- Daftar Pustaka Aps OrangDocument3 pagesDaftar Pustaka Aps OrangAlexander DickyNo ratings yet
- PT InrDocument3 pagesPT InrJeniah Lerios OcsioNo ratings yet
- Hemostatic Drugs: HennivandaDocument12 pagesHemostatic Drugs: HennivandaTasya FakhiraNo ratings yet
- Primary Hemostasis LabDocument2 pagesPrimary Hemostasis LabMara Gane100% (1)
- Tosoh HPLC G11 InstrumentDocument25 pagesTosoh HPLC G11 InstrumentHw XuNo ratings yet
- Bleeding Time PDFDocument25 pagesBleeding Time PDFKhaled ZatariNo ratings yet
- Blood Components (E-Learning Activity) : Francisco, Frances Lorraine RDocument3 pagesBlood Components (E-Learning Activity) : Francisco, Frances Lorraine RpixiedustNo ratings yet
- 3 4Document2 pages3 4cherryNo ratings yet
- Technothrombin TGA Triggers ML-00-00293REV01Document8 pagesTechnothrombin TGA Triggers ML-00-00293REV01myafiaNo ratings yet
- Disorders of HemostasisDocument50 pagesDisorders of Hemostasisalibayaty1100% (1)
- Secondary HemostasisDocument24 pagesSecondary Hemostasisalibayaty1No ratings yet
- Activated Partial Thromboplastin Time: FeatureDocument3 pagesActivated Partial Thromboplastin Time: FeatureMaria VisitacionNo ratings yet