You might also like
- 2021 - Neonatal Dermatology The Normal, The Common and The SeriousDocument14 pages2021 - Neonatal Dermatology The Normal, The Common and The SeriousnancyerlenNo ratings yet
- Csa Book MRCGP Csa Cases MRCGP CourseDocument22 pagesCsa Book MRCGP Csa Cases MRCGP CourseEshtiag43% (7)
- ENDOPHTHALMITISDocument32 pagesENDOPHTHALMITISBalaji KrishnanNo ratings yet
- Post Cataract EndophthalmitisDocument55 pagesPost Cataract Endophthalmitisdr samreen arifNo ratings yet
- Bacterial Keratitis PritiDocument58 pagesBacterial Keratitis Pritipriti08988% (8)
- Endophthalmitis: DR Santosh ChaudharyDocument38 pagesEndophthalmitis: DR Santosh Chaudharyritesh mishraNo ratings yet
- EndophthalmitisDocument51 pagesEndophthalmitisSana AzimNo ratings yet
- Keratitis PrintDocument33 pagesKeratitis PrinthamzahNo ratings yet
- Causes, Symptoms and Treatment of Blepharitis and ConjunctivitisDocument63 pagesCauses, Symptoms and Treatment of Blepharitis and Conjunctivitislailatut toriqoh100% (1)
- Endophthalmitis: DR Raheela Naz PGR Eye Unit 2Document16 pagesEndophthalmitis: DR Raheela Naz PGR Eye Unit 2Usman ImtiazNo ratings yet
- Endophthalmitis: Classification, Etiology and Clinical ApproachDocument42 pagesEndophthalmitis: Classification, Etiology and Clinical ApproachHieLdaJanuariaNo ratings yet
- EndophthalmitisDocument41 pagesEndophthalmitislishasasNo ratings yet
- Corneal Infections: HundumaDocument40 pagesCorneal Infections: HundumaHawwi IsmailNo ratings yet
- 8-Visual Cues Ophthalmology PDFDocument64 pages8-Visual Cues Ophthalmology PDFCarimaGhalieNo ratings yet
- Endophthalmitis: Original Article Contributed byDocument12 pagesEndophthalmitis: Original Article Contributed bytaufikNo ratings yet
- CD 4Document8 pagesCD 4Amira AlmutairiNo ratings yet
- Posterior Chamber of Eye Infection 1Document50 pagesPosterior Chamber of Eye Infection 1Aryan PatelNo ratings yet
- Diagnosing and Treating EndophthalmitisDocument42 pagesDiagnosing and Treating EndophthalmitisGetenet shumetNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document48 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Nauli PanjaitanNo ratings yet
- 24compl's Cataract SurgeryDocument25 pages24compl's Cataract SurgeryShari' Si WahyuNo ratings yet
- Conjunctival Diseases Presentation New Version SendDocument82 pagesConjunctival Diseases Presentation New Version Sendruhulcoc1No ratings yet
- Gabungan Materi FarmakoterapiDocument235 pagesGabungan Materi FarmakoterapiIndah PrayestiNo ratings yet
- Kelainan Uvea,: Dr. I Gede Suparta SP.MDocument14 pagesKelainan Uvea,: Dr. I Gede Suparta SP.Mbasyit bafadhalNo ratings yet
- EndophthalmitisDocument30 pagesEndophthalmitisNazmiNo ratings yet
- RED EYE WITH DECREASED VISION FixedDocument70 pagesRED EYE WITH DECREASED VISION FixedChandraNo ratings yet
- Ocular Manifestation of Hiv (Umolo) - 2Document74 pagesOcular Manifestation of Hiv (Umolo) - 2emmydomcNo ratings yet
- Preventing Blindness: Causes and Treatment of EndophthalmitisDocument18 pagesPreventing Blindness: Causes and Treatment of EndophthalmitisRhNo ratings yet
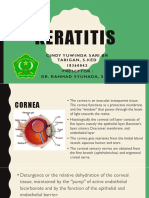
- Keratitis: Cindy Yuwindasari BR Tarigan, S.Ked 1 8 3 6 0 0 4 2 Preseptor: Dr. Rahmadsyuhada, Sp. MDocument20 pagesKeratitis: Cindy Yuwindasari BR Tarigan, S.Ked 1 8 3 6 0 0 4 2 Preseptor: Dr. Rahmadsyuhada, Sp. MTioNo ratings yet
- KeratitisDocument14 pagesKeratitismalathiNo ratings yet
- Complications of Penetrating KeratoplastyDocument105 pagesComplications of Penetrating KeratoplastyVishwajeetNo ratings yet
- Corneal UlcerDocument28 pagesCorneal Ulcerdevanand21100% (1)
- TASSDocument11 pagesTASSNike KeketNo ratings yet
- TASSDocument11 pagesTASSNike KeketNo ratings yet
- TASSDocument11 pagesTASSNike KeketNo ratings yet
- Ocular Manif. of HIVDocument75 pagesOcular Manif. of HIVPrabhjot SinghNo ratings yet
- Background: Bacterial Endophthalmitis. Retinopathy Induced by EnterococcusDocument7 pagesBackground: Bacterial Endophthalmitis. Retinopathy Induced by EnterococcusRani Henty NovitaNo ratings yet
- L9 Cataract and Ocular PharmDocument26 pagesL9 Cataract and Ocular PharmSofíaGriggsNo ratings yet
- Chlamydial Conjunctivitis GuideDocument36 pagesChlamydial Conjunctivitis GuideAsad FrazNo ratings yet
- Vision Screening in Children Allergic Conjunctivitis Corneal AbrasionDocument78 pagesVision Screening in Children Allergic Conjunctivitis Corneal AbrasionKristine VanzuelaNo ratings yet
- Coo Endophthalmitis Post-Op v9 Sept11Document2 pagesCoo Endophthalmitis Post-Op v9 Sept11Ferdinando BaehaNo ratings yet
- Endophthalmitis: Major ReviewDocument5 pagesEndophthalmitis: Major ReviewannisaNo ratings yet
- Subgroups of EndophthalmitisDocument25 pagesSubgroups of EndophthalmitisImran SyedNo ratings yet
- ConjunctivitisDocument77 pagesConjunctivitisHari GowthamNo ratings yet
- Optha SeminarDocument29 pagesOptha SeminarYoseph DemisseNo ratings yet
- Clinical Decision Making in MicrObial KeratitismainefinDocument132 pagesClinical Decision Making in MicrObial KeratitismainefinNooreen NunnooNo ratings yet
- Conjuctivitis: 1. BacterialDocument11 pagesConjuctivitis: 1. BacterialDiana TiganucNo ratings yet
- Conjunctivitis 120201025034 Phpapp02Document34 pagesConjunctivitis 120201025034 Phpapp02Ilham RafisNo ratings yet
- Kegawatdarutan Mata Dalam Konsep DogaDocument68 pagesKegawatdarutan Mata Dalam Konsep DogaDavi DzikirianNo ratings yet
- herpeticeyedisease-151106190451-lva1-app6891Document68 pagesherpeticeyedisease-151106190451-lva1-app6891Ali YılmazNo ratings yet
- The Red EyeDocument45 pagesThe Red EyeIsraa AlaaNo ratings yet
- No Endoftalmitis IncidenceDocument19 pagesNo Endoftalmitis IncidenceR.m. AndriyanNo ratings yet
- Corneal Ulcer: Prepared By: Renuka Shrestha Roll No: 29 PBBN 3rd Year SMTCDocument41 pagesCorneal Ulcer: Prepared By: Renuka Shrestha Roll No: 29 PBBN 3rd Year SMTCsushma shresthaNo ratings yet
- Soft Contact Lens Complicatioan - EditedDocument41 pagesSoft Contact Lens Complicatioan - EditedR.m. AndriyanNo ratings yet
- Conjunctivitis (Inclusion) Vs Acute Bacterial ConjunctivitisDocument13 pagesConjunctivitis (Inclusion) Vs Acute Bacterial ConjunctivitisJayricDepalobosNo ratings yet
- Ocular Emergencies DR Wisudawan SPM - KelaskedokteranDocument22 pagesOcular Emergencies DR Wisudawan SPM - KelaskedokteranMonna Medani LysabellaNo ratings yet
- 079 Muhammad Khairul Nizam Bin Khir 7.1Document30 pages079 Muhammad Khairul Nizam Bin Khir 7.1Ilham RafisNo ratings yet
- ENDOFTALMITISDocument19 pagesENDOFTALMITISAndrea ArmeriaNo ratings yet
- Clinical App Red Eye Without Blurred VisionDocument38 pagesClinical App Red Eye Without Blurred VisionPriskila SamanthaNo ratings yet
- Common Eye ConditionsDocument35 pagesCommon Eye ConditionsElukoti BhosleNo ratings yet
- MS SensesDocument13 pagesMS SensesFrechel Ann Landingin PedrozoNo ratings yet
- Endophthalmitis Clinical Practice Guidelines PDFDocument7 pagesEndophthalmitis Clinical Practice Guidelines PDFAna RicuNo ratings yet
- Endophthalmitis 1Document42 pagesEndophthalmitis 1Nasrin sultana rmcNo ratings yet
- Endophthalmitis 1Document42 pagesEndophthalmitis 1Nasrin sultana rmcNo ratings yet
- Diabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeDocument63 pagesDiabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeNear DeathNo ratings yet
- Endophthalmitis 1Document42 pagesEndophthalmitis 1Nasrin sultana rmcNo ratings yet
- Endophthalmitis 1Document42 pagesEndophthalmitis 1Nasrin sultana rmcNo ratings yet
- Endophthalmitis 1Document42 pagesEndophthalmitis 1Nasrin sultana rmcNo ratings yet
- Vomiting: Compendium (Yardley, PA) February 2009Document10 pagesVomiting: Compendium (Yardley, PA) February 2009Vini SasmitaNo ratings yet
- Occupational Therapy's Role in Managing ArthritisDocument2 pagesOccupational Therapy's Role in Managing ArthritisThe American Occupational Therapy AssociationNo ratings yet
- Assessing The NeckDocument3 pagesAssessing The NeckAnne Joyce Lara AlbiosNo ratings yet
- Spot The Difference: 1 This Diagram Shows The Male Reproductive SystemDocument3 pagesSpot The Difference: 1 This Diagram Shows The Male Reproductive SystemPedroDavid JoaquinFernandoNo ratings yet
- B Cell Cytokine SDocument11 pagesB Cell Cytokine Smthorn1348No ratings yet
- Proposal of MulumebetDocument40 pagesProposal of MulumebetMulumebet EshetuNo ratings yet
- ORS Package InsertDocument2 pagesORS Package InsertJan Aira Almazan100% (1)
- 208-230 CH08 Lowdermilk - QXDDocument23 pages208-230 CH08 Lowdermilk - QXDSyarifah Ro'fahNo ratings yet
- Trauma Module FinalDocument34 pagesTrauma Module FinalMarian YuqueNo ratings yet
- The Emotion Code Has Helped Trapped EmotionsDocument2 pagesThe Emotion Code Has Helped Trapped Emotionsmagdalena0% (1)
- Hema I Chapter 11 - RBC IndicesDocument15 pagesHema I Chapter 11 - RBC IndicesKumneger DereseNo ratings yet
- 2019-02-27T205056.849Document3 pages2019-02-27T205056.849writer topNo ratings yet
- Carilion Clinic 2018 Fact SheetDocument2 pagesCarilion Clinic 2018 Fact Sheetphv209No ratings yet
- Lecture ISK UKI - Dr. Sahala Panggabean SP - PDDocument25 pagesLecture ISK UKI - Dr. Sahala Panggabean SP - PDBen HonorseekerNo ratings yet
- Foreseeable Crisis PlanDocument6 pagesForeseeable Crisis PlanGladys JhayeNo ratings yet
- Modifikasi Formula Enteral Rumah Sakit Siap SeduhDocument8 pagesModifikasi Formula Enteral Rumah Sakit Siap SeduhAsfi Ni'amNo ratings yet
- Medicine OSCE LatestDocument231 pagesMedicine OSCE LatestPrasad HewawasamNo ratings yet
- English For Nursing Topic 13 Reinforcing A Dietary ProgramDocument7 pagesEnglish For Nursing Topic 13 Reinforcing A Dietary ProgramAyu AndiniiNo ratings yet
- 2010 - 2016 With AnswersDocument806 pages2010 - 2016 With AnswersIbrahim Abueltaif83% (6)
- ACOG All About Exercise During PregnancyDocument4 pagesACOG All About Exercise During PregnancyriasahNo ratings yet
- Paper 3 Argumentative Essay Alexis-2Document9 pagesPaper 3 Argumentative Essay Alexis-2api-314832012No ratings yet
- Arul Kumar An 2013Document10 pagesArul Kumar An 2013Silvana ReyesNo ratings yet
- Guillain Barre SyndromeDocument43 pagesGuillain Barre Syndromegabrielle magdaraogNo ratings yet
- Praktek Essentials: Tanda Dan GejalaDocument5 pagesPraktek Essentials: Tanda Dan GejalaElvis HusainNo ratings yet
- Surgery II - Topical Past Papers (2007-2019)Document61 pagesSurgery II - Topical Past Papers (2007-2019)AnmahNo ratings yet
- Subject Final FSDocument42 pagesSubject Final FSbangladeshusembassyNo ratings yet
- FISA Engl DISCIPLINA FIZIOLOGIE I MODUL LIMBA ENGLEZADocument8 pagesFISA Engl DISCIPLINA FIZIOLOGIE I MODUL LIMBA ENGLEZAAbdallah Darwish100% (1)
- Lesson Plan On RhinitisDocument15 pagesLesson Plan On Rhinitiskiran mahal100% (4)