You might also like
- ECG Master Class-1Document132 pagesECG Master Class-1Shohag ID Center100% (1)
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasFrom EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasRating: 5 out of 5 stars5/5 (2)
- Poster2 Arrhythmia Recognition eDocument1 pagePoster2 Arrhythmia Recognition eItharshan IndreswaranNo ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Critical Care NursingDocument159 pagesCritical Care NursingJoy Jarin50% (2)
- ECG WorldDocument139 pagesECG WorldsatyaNo ratings yet
- Ecg WorkshopDocument39 pagesEcg WorkshopUber SnooferNo ratings yet
- ACLS Exam ADocument8 pagesACLS Exam ASean Johnson83% (30)
- ECG InterpretationDocument1 pageECG InterpretationCecil-An DalanonNo ratings yet
- Ecg NoobsDocument103 pagesEcg NoobsGhaidaa Sadeq100% (1)
- ECG & ArrhythmiasDocument8 pagesECG & ArrhythmiasDr. SobanNo ratings yet
- BTKV - Cardiac - Carpentier's Reconstructive Valve SurgeryDocument363 pagesBTKV - Cardiac - Carpentier's Reconstructive Valve SurgeryDavid Christian100% (1)
- ECG BasicsDocument34 pagesECG BasicsBeaCeeNo ratings yet
- Basic ECG For ParamedicDocument82 pagesBasic ECG For ParamedicMaza AmfoterikNo ratings yet
- Pediatrics ECG by DR Ali Bel KheirDocument9 pagesPediatrics ECG by DR Ali Bel KheirFerasNo ratings yet
- Ecg / EkgDocument10 pagesEcg / EkgSilver Villota Magday Jr.No ratings yet
- ECG Normal and AbnormalDocument74 pagesECG Normal and Abnormalawaniedream8391100% (1)
- Electrocardiogram (ECG/EKG) : Jovel Balaba Tangonan InstructorDocument77 pagesElectrocardiogram (ECG/EKG) : Jovel Balaba Tangonan InstructorNecky AlbaciteNo ratings yet
- ECG InterpretationDocument11 pagesECG InterpretationAndrea AndradaNo ratings yet
- Normal ECGDocument41 pagesNormal ECGRoscelie KhoNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Ecg 01Document103 pagesEcg 01Bandar al ghamdi100% (2)
- Temporary Pacemakers-SICU's 101 PrimerDocument51 pagesTemporary Pacemakers-SICU's 101 Primerwaqas_xsNo ratings yet
- Sally Aburumman Bushra SaleemDocument75 pagesSally Aburumman Bushra SaleemAbdulrahman AlsayyedNo ratings yet
- Ecg PDFDocument70 pagesEcg PDFlauras3005No ratings yet
- ECG ArrythemiaDocument79 pagesECG ArrythemiaMahadevNo ratings yet
- Case StudyDocument34 pagesCase StudyBSNNursing101No ratings yet
- Principles of ECGDocument11 pagesPrinciples of ECGDeinielle Magdangal RomeroNo ratings yet
- Sindromul Coronarian Acut: UMF VB Timisoara Departamentul VI Medicina Interna de AmbulatorDocument78 pagesSindromul Coronarian Acut: UMF VB Timisoara Departamentul VI Medicina Interna de AmbulatorIulia CeveiNo ratings yet
- Basics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyDocument206 pagesBasics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyRavi SharmaNo ratings yet
- Basic of EcgDocument82 pagesBasic of Ecgpopescuioana1No ratings yet
- Arrhythmia: PalpitationDocument36 pagesArrhythmia: PalpitationHala BahaaNo ratings yet
- Ecg Guidelines: Donna J. Castillo, MDDocument76 pagesEcg Guidelines: Donna J. Castillo, MDBheck Magat100% (1)
- A Guide To: Noob'SDocument103 pagesA Guide To: Noob'STeodorescu Claudia GabrielaNo ratings yet
- Hotel Dpalma, Bandung 16 Maret 2018: Dr. Benny Prasetya PDocument145 pagesHotel Dpalma, Bandung 16 Maret 2018: Dr. Benny Prasetya PkangheriNo ratings yet
- NEONARYTDocument28 pagesNEONARYToctaviena zakariaNo ratings yet
- Basics of ECG (Dr. MD Kalimuddin)Document53 pagesBasics of ECG (Dr. MD Kalimuddin)CloudySkyNo ratings yet
- ECG For BeginnersDocument61 pagesECG For Beginnersblndffl100% (2)
- Ecg 1Document198 pagesEcg 1hibaNo ratings yet
- How To Read An EKG StripDocument9 pagesHow To Read An EKG StripRavi PandeNo ratings yet
- ECG PresentationDocument52 pagesECG PresentationShah NahidNo ratings yet
- Ipd Kuliah Ekg Blok KegawatdaruratanDocument118 pagesIpd Kuliah Ekg Blok Kegawatdaruratansiti solikhaNo ratings yet
- Ecg FileDocument29 pagesEcg Fileneha miriNo ratings yet
- ECG 22septDocument53 pagesECG 22septA ScribbbNo ratings yet
- Kamis 10 September 2015 - IPD 2 - Kuliah-Ekg-Blok-KegawatdaruratanDocument118 pagesKamis 10 September 2015 - IPD 2 - Kuliah-Ekg-Blok-KegawatdaruratanIrfanArifZulfikarNo ratings yet
- ECG Tutorial - Basic Principles of ECG Analysis - UpToDateDocument17 pagesECG Tutorial - Basic Principles of ECG Analysis - UpToDateImja94No ratings yet
- 01 - Basic Principles of ECG Analysis - UpToDateDocument22 pages01 - Basic Principles of ECG Analysis - UpToDateElmer MoscosoNo ratings yet
- ECG Intro With Ref To QT Interval FinalDocument59 pagesECG Intro With Ref To QT Interval FinalGeorge VergheseNo ratings yet
- Introduction To ECGDocument39 pagesIntroduction To ECGSingey LhendupNo ratings yet
- DrAbnet ECG - BasicsDocument99 pagesDrAbnet ECG - BasicsAbnet WondimuNo ratings yet
- Ecg PreparationDocument15 pagesEcg PreparationErika Danalle ArceoNo ratings yet
- Electrocardiogram (ECG)Document25 pagesElectrocardiogram (ECG)Laraib KanwalNo ratings yet
- Electrocardiograph Y: Dr. Fatimah Eliana, SPPD, Kemd, FinasimDocument118 pagesElectrocardiograph Y: Dr. Fatimah Eliana, SPPD, Kemd, FinasimTommy WidjayaNo ratings yet
- ECG Approach by DR SSSDocument51 pagesECG Approach by DR SSSAritro DasguptaNo ratings yet
- How To Read An ECGDocument21 pagesHow To Read An ECGSlychenkoNo ratings yet
- Ekg PJKDocument113 pagesEkg PJKdevipuspaNo ratings yet
- The ElectrocardiogramDocument53 pagesThe ElectrocardiogramJEM93No ratings yet
- ECG PracticalDocument48 pagesECG PracticalbvkjtzrvnyNo ratings yet
- ElectrocardiographyDocument4 pagesElectrocardiographyJho BuanNo ratings yet
- Interpretasi ElektrokardiografiDocument60 pagesInterpretasi ElektrokardiografiYogi GustriansyahNo ratings yet
- ECGDocument33 pagesECGWasif RaheelNo ratings yet
- EcgDocument11 pagesEcgRajneesh TiwariNo ratings yet
- Approach To A Patient With PR Interval AbnormalitiesDocument20 pagesApproach To A Patient With PR Interval AbnormalitiesToufiqurRahmanNo ratings yet
- Basic ECG Interpretation NCM 112 LEILADocument80 pagesBasic ECG Interpretation NCM 112 LEILALui Andrei AnilaNo ratings yet
- What Is The Definition of Electrocardiogram/ECG?Document4 pagesWhat Is The Definition of Electrocardiogram/ECG?Kyle AndrewNo ratings yet
- HYPERTENSION+QUESTIONNAIRE+ (Rev 1+2012) PDFDocument1 pageHYPERTENSION+QUESTIONNAIRE+ (Rev 1+2012) PDFZito AmoraNo ratings yet
- Hands-Only CPR: Additional Information For InstructorsDocument2 pagesHands-Only CPR: Additional Information For InstructorsM ANo ratings yet
- Left Anterior Fascicular Block (LAFB) ECG Review - Criteria and ExamplesDocument1 pageLeft Anterior Fascicular Block (LAFB) ECG Review - Criteria and ExamplesWiwik Puji LestariNo ratings yet
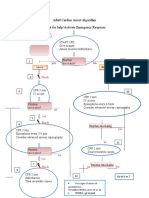
- Adult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseDocument1 pageAdult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseICU RSBMNo ratings yet
- Braunwald Lecture Series #2Document33 pagesBraunwald Lecture Series #2usfcards100% (2)
- Farmacology Del Paro CardiacoDocument14 pagesFarmacology Del Paro CardiacoNicoSwtifNo ratings yet
- PowerpointDocument12 pagesPowerpointapi-585922320No ratings yet
- Heart Murmurs: What Is A Heart Murmur?Document2 pagesHeart Murmurs: What Is A Heart Murmur?Stefan Codrin CriclevitzNo ratings yet
- Diagnosis and Management Sudden Cardiac Death 2005Document7 pagesDiagnosis and Management Sudden Cardiac Death 2005aminceloNo ratings yet
- Obstetric Anesthesia Management of The Patient With Cardiac DiseaseDocument13 pagesObstetric Anesthesia Management of The Patient With Cardiac DiseaseRicardoNo ratings yet
- List New Cath LabDocument3 pagesList New Cath LabtazkiaNo ratings yet
- Antianginal Drugs: Dr. Jim AmisiDocument11 pagesAntianginal Drugs: Dr. Jim AmisiMike AnnisNo ratings yet
- Cardiopulmonary Resuscitation (CPR) : ImportanceDocument19 pagesCardiopulmonary Resuscitation (CPR) : Importancesxm2901No ratings yet
- Myocardial Diseases: Marvi G. Dulnuan - Niog, MD, FPSPDocument94 pagesMyocardial Diseases: Marvi G. Dulnuan - Niog, MD, FPSPLianne LagayanNo ratings yet
- Daftar Pustaka: Universitas Sumatera UtaraDocument3 pagesDaftar Pustaka: Universitas Sumatera UtaraAdisti ZakyatunnisaNo ratings yet
- Peadiatric ECGDocument54 pagesPeadiatric ECGshalini0580% (5)
- Pembicara: Dr. Orfeas Liangos - Coburg GermanyDocument6 pagesPembicara: Dr. Orfeas Liangos - Coburg GermanyRicky VirnardoNo ratings yet
- Mitral ValveDocument48 pagesMitral Valvestoicea_katalinNo ratings yet
- Circulationaha 119 043780Document2 pagesCirculationaha 119 043780Robby Paguh TariganNo ratings yet
- Data Offline Surveilans PTM Berbasis FKTP: Tanggal PemeriksaanDocument29 pagesData Offline Surveilans PTM Berbasis FKTP: Tanggal Pemeriksaansri setyowatiNo ratings yet
- Hafiz Abdul Rehman (1) - CompressedDocument1 pageHafiz Abdul Rehman (1) - CompressedFaisal BasharatNo ratings yet
- Case Reports AbstractsDocument7 pagesCase Reports AbstractsNovie AstiniNo ratings yet
- Cardiac Assessment: Sickkids Advanced Paediatric Cardiology ProgramDocument61 pagesCardiac Assessment: Sickkids Advanced Paediatric Cardiology Programmadimadi11No ratings yet
- Sample Writing Task 3: Time Allowed: 40 MinutesDocument3 pagesSample Writing Task 3: Time Allowed: 40 Minutesprakash poudelNo ratings yet