You might also like
- Atrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesFrom EverandAtrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesRating: 4 out of 5 stars4/5 (1)
- Anti-anginal Drugs Guide to Key MedicationsDocument16 pagesAnti-anginal Drugs Guide to Key MedicationsrizkyNo ratings yet
- Anti AnginaDocument16 pagesAnti AnginaAik NoeraNo ratings yet
- Pharmacology AnginaDocument28 pagesPharmacology AnginaalijanmarwatNo ratings yet
- Angina Set #8Document26 pagesAngina Set #8Zaid Al-KadhimiNo ratings yet
- Anti Anginal DrugsDocument26 pagesAnti Anginal DrugsAtharva PuranikNo ratings yet
- Antinanginal DrugsDocument43 pagesAntinanginal DrugsHUZAIFA YAMAANNo ratings yet
- Antianginal DrugsDocument21 pagesAntianginal DrugsMaryam Shoukat Ali100% (1)
- Cardiac PharmDocument6 pagesCardiac PharmJohn SmithNo ratings yet
- Pharmacology of Angina Pectoris: Types, Classification of Drugs, and Mechanism of ActionDocument11 pagesPharmacology of Angina Pectoris: Types, Classification of Drugs, and Mechanism of ActionZakarie Abdullahi HusseinNo ratings yet
- Antianginal ClassDocument32 pagesAntianginal ClassAnonymous whcvnPBeQNo ratings yet
- Anti Anginal DrugsDocument33 pagesAnti Anginal DrugsMuhammad AhmadNo ratings yet
- DR - Datten Bangun MSC - SPFK & DR - Tri Widyawati Msi, PHD Dept - Farmakologi & Therapeutik Fak - Kedokteran Usu MedanDocument50 pagesDR - Datten Bangun MSC - SPFK & DR - Tri Widyawati Msi, PHD Dept - Farmakologi & Therapeutik Fak - Kedokteran Usu MedanHabib Al KahfiNo ratings yet
- Angina NursingDocument62 pagesAngina NursingNikita JangraNo ratings yet
- Pharmacology Misbah PDFDocument238 pagesPharmacology Misbah PDFRiham Khamis86% (7)
- Angina Pectoris & Anti Anginal DrugsDocument46 pagesAngina Pectoris & Anti Anginal DrugsMohammad AliNo ratings yet
- Antianginal 171115034620Document34 pagesAntianginal 171115034620benny christantoNo ratings yet
- Anti Angina (Hany)Document51 pagesAnti Angina (Hany)Angga AhadiyatNo ratings yet
- Anti - Anginal MedicationDocument41 pagesAnti - Anginal MedicationShine StephenNo ratings yet
- Pharmacology of Ischemic Heart DiseaseDocument51 pagesPharmacology of Ischemic Heart DiseaseabenezergebrekirstosNo ratings yet
- Anti-Angina Drugs for Chest Pain ReliefDocument60 pagesAnti-Angina Drugs for Chest Pain ReliefPranish SawantNo ratings yet
- Nursing Care of Clients With Cardiovascular DisorderDocument16 pagesNursing Care of Clients With Cardiovascular DisorderLuna MarieNo ratings yet
- Anti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistDocument25 pagesAnti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistpradeephdNo ratings yet
- Anti-Anginal Drugs ExplainedDocument19 pagesAnti-Anginal Drugs ExplainedAnusha ZubairNo ratings yet
- Drugs Used in Myocardial InfarctionDocument53 pagesDrugs Used in Myocardial InfarctionSandeep KannegantiNo ratings yet
- HypertensionDocument29 pagesHypertensionkadir.dallenmae.d.bcsiNo ratings yet
- Ischemic Heart DiseaseDocument31 pagesIschemic Heart DiseaseRohit SahNo ratings yet
- III) Pharmacotherapy of Angina PectorisDocument23 pagesIII) Pharmacotherapy of Angina PectorisAyro Business CenterNo ratings yet
- Calcium Channel Blocker (CCB)Document36 pagesCalcium Channel Blocker (CCB)Nafisa TasnimNo ratings yet
- Anoosha Roll#21Document19 pagesAnoosha Roll#21Anusha ZubairNo ratings yet
- Drugs Acting On Cardio Vascular SystemDocument16 pagesDrugs Acting On Cardio Vascular SystemANUSHYA B PSGRKCWNo ratings yet
- Calcium Channel MedicationsDocument17 pagesCalcium Channel MedicationsMarriette Bayaya AntiquinaNo ratings yet
- Drugs Affecting Cardiac and Renal Systems: Jan Bazner-Chandler MSN, CNS, C-PNP, RNDocument70 pagesDrugs Affecting Cardiac and Renal Systems: Jan Bazner-Chandler MSN, CNS, C-PNP, RNromeorobin07No ratings yet
- Pharmacology of Anti Hypertensive Agents (For BPT Students)Document17 pagesPharmacology of Anti Hypertensive Agents (For BPT Students)Dr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Antianginal Drugs: - Organic Nitrates - Calcium Channel BlockersDocument30 pagesAntianginal Drugs: - Organic Nitrates - Calcium Channel BlockersBenny TrisaktyariNo ratings yet
- Module 3.3 - CardioDocument12 pagesModule 3.3 - CardioCatherine Sinen ObinqueNo ratings yet
- Drugs of CvsDocument32 pagesDrugs of CvsAgus HaryantoNo ratings yet
- Lecture 8 Heart FailureDocument38 pagesLecture 8 Heart Failureukashazam19No ratings yet
- Chapter 37 Cardiac Glycosides Antianginals and AntidysrhythmicsDocument5 pagesChapter 37 Cardiac Glycosides Antianginals and AntidysrhythmicsErika Joy Cabison TamayoNo ratings yet
- Obat Gagal Jantung N Anti AnginaDocument42 pagesObat Gagal Jantung N Anti AnginaAyu Devi YantiNo ratings yet
- Cardiovascular Drugs: Dr. Hazha S. Ameen MSCDocument25 pagesCardiovascular Drugs: Dr. Hazha S. Ameen MSCAhmed MohamadNo ratings yet
- Drugs For CHF & Angina PDFDocument15 pagesDrugs For CHF & Angina PDFAbdullah ElsayedNo ratings yet
- Angina PectorisDocument24 pagesAngina PectorisAshwin Raghav SankarNo ratings yet
- CONGESTIVE HEART FAILURE - New-1Document32 pagesCONGESTIVE HEART FAILURE - New-1Agus SuprionoNo ratings yet
- Angina PectorisDocument31 pagesAngina Pectorisamjad.46987No ratings yet
- Antianginal DrugsDocument32 pagesAntianginal Drugssultan khabeebNo ratings yet
- Anti AnginaDocument5 pagesAnti Anginalandita683No ratings yet
- Treatment of Angina Pectoris-2Document19 pagesTreatment of Angina Pectoris-2Habib UllahNo ratings yet
- Cardio CHF Angina Drugs MegDocument3 pagesCardio CHF Angina Drugs MegJhonny pingolNo ratings yet
- Angina Types and TreatmentDocument44 pagesAngina Types and TreatmentsimonjosanNo ratings yet
- Erasmus Heart DrugsDocument90 pagesErasmus Heart DrugsDanilo ČešljaracNo ratings yet
- AnginaDocument16 pagesAnginaMc_Lopez_1761No ratings yet
- Cardiac DrugsDocument21 pagesCardiac DrugsMona MahfouzNo ratings yet
- Antianginal Drugs DR Hussam 2023Document12 pagesAntianginal Drugs DR Hussam 2023ManWol JangNo ratings yet
- Pharmacology N23 Group2Document4 pagesPharmacology N23 Group2Andrie JaraveloNo ratings yet
- Angina PectorisDocument24 pagesAngina PectorisAyu PurbaNo ratings yet
- 6 AntianginalDocument38 pages6 AntianginalAyush GuptaNo ratings yet
- Angina Pectoris: Coronary Heart Disease. Myocardial Ischemia, Stable AnginaDocument3 pagesAngina Pectoris: Coronary Heart Disease. Myocardial Ischemia, Stable AnginaYudia MahardikaNo ratings yet
- Antibacterials CMDocument72 pagesAntibacterials CMMike AnnisNo ratings yet
- Antihemintic DrugsDocument24 pagesAntihemintic DrugsMike AnnisNo ratings yet
- Analgesic Drugs: Dr. Jim AmisiDocument65 pagesAnalgesic Drugs: Dr. Jim AmisiMike AnnisNo ratings yet
- Anticoagulants: Dr. Jim AmisiDocument51 pagesAnticoagulants: Dr. Jim AmisiMike AnnisNo ratings yet
- National Clinical Guidelines For Management of Diabetes Melitus - CompleteDocument73 pagesNational Clinical Guidelines For Management of Diabetes Melitus - CompleteLaurensia Erlina Natalia100% (1)
- BSCM234 T2-2020 Lesson 5Document83 pagesBSCM234 T2-2020 Lesson 5Mike AnnisNo ratings yet
- BSCM 234 T2 Lesson 7Document53 pagesBSCM 234 T2 Lesson 7Mike AnnisNo ratings yet
- BSCM 234 Lesson 2-1Document47 pagesBSCM 234 Lesson 2-1Mike AnnisNo ratings yet
- BSCM 234 T2-2020 Lesson 4Document77 pagesBSCM 234 T2-2020 Lesson 4Mike AnnisNo ratings yet
- BSCM 234: Disaster ManagementDocument41 pagesBSCM 234: Disaster ManagementMike AnnisNo ratings yet
- BSCM234 T2-2020 Lesseon 1-1Document52 pagesBSCM234 T2-2020 Lesseon 1-1Mike AnnisNo ratings yet
- BSCM 234T2 Lesson 6Document60 pagesBSCM 234T2 Lesson 6Mike AnnisNo ratings yet
- Histology of Urinary SystemDocument35 pagesHistology of Urinary SystemMike AnnisNo ratings yet
- BSCM 234 Disaster Management (2CRS)Document4 pagesBSCM 234 Disaster Management (2CRS)Mike AnnisNo ratings yet
- Amino Acids OverviewDocument30 pagesAmino Acids OverviewbrownhazelNo ratings yet
- Health Behaviour: Current Issues and ChallengesDocument13 pagesHealth Behaviour: Current Issues and ChallengesK.A.No ratings yet
- Agco - DBB - f68.f69Document6 pagesAgco - DBB - f68.f69Mohd Khairi Mohd NorzianNo ratings yet
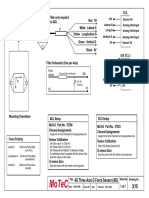
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- BKTK-2010, Failure in Material ConstructionsDocument17 pagesBKTK-2010, Failure in Material ConstructionsSorulay Way-neyNo ratings yet
- National Coalition For The HomelessDocument7 pagesNational Coalition For The HomelessLee GaylordNo ratings yet
- Volcanic Eruption Types and ProcessDocument18 pagesVolcanic Eruption Types and ProcessRosemarie Joy TanioNo ratings yet
- Payroll Accounting 2015 1st Edition Landin Test Bank 1Document106 pagesPayroll Accounting 2015 1st Edition Landin Test Bank 1dorothy100% (47)
- The Strange ICA Stones of PeruDocument31 pagesThe Strange ICA Stones of PeruRoman Aleshkevich100% (1)
- Flame Amplifier HoneywellDocument8 pagesFlame Amplifier Honeywellgavo vargoNo ratings yet
- Group 3Document11 pagesGroup 3Sharp MIER TVNo ratings yet
- Introducion To Load Cells UtilcellDocument22 pagesIntroducion To Load Cells UtilcellRifi MohamedNo ratings yet
- D1553.140U1 German Braun Speed - Braun Card-Xi'an Yuanhua Instrument Co., LTDDocument2 pagesD1553.140U1 German Braun Speed - Braun Card-Xi'an Yuanhua Instrument Co., LTDTrong Hung NguyenNo ratings yet
- Smart medical system monitors dementia patients' medicationDocument9 pagesSmart medical system monitors dementia patients' medicationKresnaNo ratings yet
- Opening SpeechDocument1 pageOpening SpeechTaniușa SavaNo ratings yet
- Bonanza A36 ChecklistDocument10 pagesBonanza A36 Checklistalbucur100% (4)
- Piriformis MuscleDocument3 pagesPiriformis MuscleBen CampbellNo ratings yet
- 6 DLL HOPE 3 2019-2020 JulyDocument2 pages6 DLL HOPE 3 2019-2020 JulyCelia BautistaNo ratings yet
- 4-Ingredient Vegan Easy Brownies - Minimalist Baker RecipesDocument2 pages4-Ingredient Vegan Easy Brownies - Minimalist Baker RecipespeteNo ratings yet
- Traits and BehaviorDocument8 pagesTraits and BehaviorNorwafa Cariga EspinosaNo ratings yet
- Childrens VoiceDocument26 pagesChildrens VoiceMira Alaa100% (2)
- Wolf Gone Wild - Juliette CrossDocument312 pagesWolf Gone Wild - Juliette CrossAbdelhediNo ratings yet
- Lodging EstablishmentsDocument2 pagesLodging EstablishmentsMich A. Gonzales0% (1)
- Supra 644, 744, 844 Beginning With Serial# Hfy90593608 - Sunbelt ...Document68 pagesSupra 644, 744, 844 Beginning With Serial# Hfy90593608 - Sunbelt ...Glacial100% (1)
- Blood Bank Case Study 5bDocument2 pagesBlood Bank Case Study 5bbalqis jaberNo ratings yet
- CardiovascularDocument155 pagesCardiovascularEric VeranoNo ratings yet
- Urban Heat Island effect document answersDocument4 pagesUrban Heat Island effect document answersAlainDelonTahilLanaNo ratings yet
- Ecl7000 enDocument2 pagesEcl7000 ensuchaya tupyangNo ratings yet
- 4 Dec - Elis Vs ElisDocument6 pages4 Dec - Elis Vs ElisRichard TenorioNo ratings yet
- 3023 History Cuisine WorksheetDocument6 pages3023 History Cuisine WorksheetFlor HenríquezNo ratings yet
- Practicum HandbookDocument12 pagesPracticum HandbookChikezie NwankworNo ratings yet