You might also like
- CIR vs. Primetown Property GroupDocument2 pagesCIR vs. Primetown Property GroupElaine Belle OgayonNo ratings yet
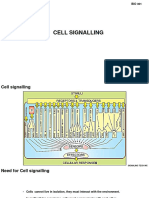
- Ch5 Cell SignallingDocument50 pagesCh5 Cell SignallingShatha KhzaimiahNo ratings yet
- NeurotransmittersDocument92 pagesNeurotransmittersClare DucutNo ratings yet
- Summary of John D. Preston, John H. O'Neal, Mary C. Talaga & Bret A. Moore's Handbook of Clinical Psychopharmacology for TherapistsFrom EverandSummary of John D. Preston, John H. O'Neal, Mary C. Talaga & Bret A. Moore's Handbook of Clinical Psychopharmacology for TherapistsNo ratings yet
- Anna Kornbluh - Marxist Film Theory and Fight Club (2019, Bloomsbury Academic)Document195 pagesAnna Kornbluh - Marxist Film Theory and Fight Club (2019, Bloomsbury Academic)Yunus ErdoğanNo ratings yet
- Receptor Mechanisms: - Receptor Are Proteins With High Affinity To ADocument45 pagesReceptor Mechanisms: - Receptor Are Proteins With High Affinity To AbevorsiNo ratings yet
- Drug-Receptor Interactions AND Pharmacodynamics: Ramla KashifDocument36 pagesDrug-Receptor Interactions AND Pharmacodynamics: Ramla KashifRamla KashifNo ratings yet
- Receptors IntroductionDocument53 pagesReceptors IntroductionSunilNo ratings yet
- Drug Receptor Bonding Signal Transduction 05mars2012 10Document34 pagesDrug Receptor Bonding Signal Transduction 05mars2012 10Yatish KarjekarNo ratings yet
- Ronald Couture - The Essential Mini-Guide To Progressive Rock (2008)Document47 pagesRonald Couture - The Essential Mini-Guide To Progressive Rock (2008)tventuraNo ratings yet
- Signal Transduction Mechanisms and Cellular ResponsesDocument39 pagesSignal Transduction Mechanisms and Cellular ResponsesBellony Sanders100% (1)
- Intracellular SignallingDocument45 pagesIntracellular Signallingsana iqbalNo ratings yet
- Molecular Mechanisms of Drug ActionDocument76 pagesMolecular Mechanisms of Drug ActionSunil100% (1)
- Cell SignalingDocument53 pagesCell SignalingKaushiki KalravNo ratings yet
- Molecular Drug Binding PrinciplesDocument100 pagesMolecular Drug Binding PrinciplesagnespaungNo ratings yet
- Neurotransmitters 1Document23 pagesNeurotransmitters 1Preety ShresthaNo ratings yet
- Mtm800 Enh Tetra Mobile Terminal 806-870 MHZ (Mt912M) : Part Number: 6866539D32-ADocument225 pagesMtm800 Enh Tetra Mobile Terminal 806-870 MHZ (Mt912M) : Part Number: 6866539D32-AThanh Kieu Tien100% (1)
- CPE655 Solid Waste ManagementDocument108 pagesCPE655 Solid Waste ManagementAmirah SufianNo ratings yet
- NuisancesDocument64 pagesNuisancesMicah Jamero FelisildaNo ratings yet
- Cell ReceptorsDocument10 pagesCell ReceptorsMaria PavalNo ratings yet
- Awareness on Waste Management of StudentsDocument48 pagesAwareness on Waste Management of StudentsJosenia Constantino87% (23)
- Al WakalahDocument12 pagesAl WakalahMahyuddin Khalid100% (3)
- Cell Signaling I: Signal Transduction & Short-term Cellular ResponsesDocument40 pagesCell Signaling I: Signal Transduction & Short-term Cellular ResponsesRNo ratings yet
- Unacademy 1Document18 pagesUnacademy 1ANUPAM ANAND KUMAR PANDEY MBA-INo ratings yet
- Chapter 21 Intro To CNS PharmaDocument8 pagesChapter 21 Intro To CNS PharmaChristine Annmarie TapawanNo ratings yet
- Cell Bio 5 Cell Communication 2021 PDFDocument31 pagesCell Bio 5 Cell Communication 2021 PDFaboodmr8nblahNo ratings yet
- ENDOCRIOLOGYDocument138 pagesENDOCRIOLOGYAqurate BuildersNo ratings yet
- Receptor-Ligand Interactions - Cell Signaling, Adhesion, Motility, Cell MigrationDocument31 pagesReceptor-Ligand Interactions - Cell Signaling, Adhesion, Motility, Cell MigrationLeebo PinPinNo ratings yet
- Advanced molecular neuropharmacology focuses on drug interactionsDocument47 pagesAdvanced molecular neuropharmacology focuses on drug interactionsimtiajahmed fahimNo ratings yet
- Drug Targets 1Document9 pagesDrug Targets 1laaraybmehmood1503No ratings yet
- ACyMSC - 05-Intracellular ReceptorsDocument38 pagesACyMSC - 05-Intracellular ReceptorsEsther NavarroNo ratings yet
- Mechanism of Drug ActionDocument24 pagesMechanism of Drug ActionBandita Datta100% (1)
- Week 3 Cell Communication 2023Document35 pagesWeek 3 Cell Communication 2023Hashley CastellyNo ratings yet
- Cell Signaling: Signaling Molecules and Their ReceptorsDocument49 pagesCell Signaling: Signaling Molecules and Their ReceptorsDeepanshu rawatNo ratings yet
- RollNo - 02 CMP Cell SignallingDocument55 pagesRollNo - 02 CMP Cell SignallingJayesh KadamNo ratings yet
- Molecular Cell Biology Prof. D. Karunagaran Department of Biotechnology Indian Institute of Technology MadrasDocument11 pagesMolecular Cell Biology Prof. D. Karunagaran Department of Biotechnology Indian Institute of Technology Madrasapi-256504985No ratings yet
- Signal and Signal Transduction For Mbs1 2014Document52 pagesSignal and Signal Transduction For Mbs1 2014Jefri SandikaNo ratings yet
- Cell Signalling BasicsDocument26 pagesCell Signalling Basics6ypywxdqmkNo ratings yet
- Membrane Proteins - Signaling Molecules and Receptors v2Document67 pagesMembrane Proteins - Signaling Molecules and Receptors v2Talha KhanNo ratings yet
- 3,4-Receptors As Drug TargetsDocument166 pages3,4-Receptors As Drug TargetsyudenfranciscoNo ratings yet
- Nuclear Receptors as Ligand-Dependent Transcription FactorsDocument21 pagesNuclear Receptors as Ligand-Dependent Transcription Factorsyousef sarairehNo ratings yet
- Receptors & Signal TransductionDocument10 pagesReceptors & Signal TransductionArslan SaeedNo ratings yet
- Biocehem AssignDocument47 pagesBiocehem Assignwendemeneh abateNo ratings yet
- Pharmacodynamics: Digvijaya Lecturer School of Medical & Allied Sciences GD Goenka UniversityDocument64 pagesPharmacodynamics: Digvijaya Lecturer School of Medical & Allied Sciences GD Goenka UniversityDigvijayaNo ratings yet
- Medicinal Chemistry:-Receptors:-: LigandDocument9 pagesMedicinal Chemistry:-Receptors:-: LigandgalooangelNo ratings yet
- Pharmaco DynamicsDocument65 pagesPharmaco Dynamicsorogadejulius5050No ratings yet
- Pharmacodynamics of Drug ReceptorsDocument11 pagesPharmacodynamics of Drug ReceptorsMandyNo ratings yet
- Mechanisms of Drug ActionDocument29 pagesMechanisms of Drug ActionKAMAU FRANCIS GATHUTHINo ratings yet
- #03 Signaling Mechanism Pharmacodynamics Vers 2Document57 pages#03 Signaling Mechanism Pharmacodynamics Vers 2tasnemaldaherNo ratings yet
- Pharmacodynamics: Principle of Drug ActionDocument55 pagesPharmacodynamics: Principle of Drug ActionFeranmi AdekunleNo ratings yet
- FarmakodinamikDocument44 pagesFarmakodinamikHarri HardiNo ratings yet
- Endocrine Biochemistry: Hormone Classification and MechanismsDocument130 pagesEndocrine Biochemistry: Hormone Classification and MechanismsDessu AshagrieNo ratings yet
- Intercellular Communication: Chemical Messengers and ReceptorsDocument30 pagesIntercellular Communication: Chemical Messengers and ReceptorsO'Brien AlfredNo ratings yet
- Lect. 10Document27 pagesLect. 10أحمدشريفNo ratings yet
- Cell Communications and Signal Transduction: Biokimia Dan Biologi Molekuler FK UntarDocument112 pagesCell Communications and Signal Transduction: Biokimia Dan Biologi Molekuler FK UntarAlbert TandyNo ratings yet
- CH1131 - Biomolecular Engineering - Week 5 - Signaling - Sep 08 15 2015Document29 pagesCH1131 - Biomolecular Engineering - Week 5 - Signaling - Sep 08 15 2015joshuaNo ratings yet
- Mekanisme Kerja Hormon Dan ReseptorDocument44 pagesMekanisme Kerja Hormon Dan ReseptorOriza Rifki RamadanNo ratings yet
- RECEPTORSDocument18 pagesRECEPTORSblessing akataNo ratings yet
- 126-Article Text-513-1-10-20170524Document10 pages126-Article Text-513-1-10-20170524Yosia KevinNo ratings yet
- Genome Size & Organization, & Gene Regulation in ProkaryotesDocument21 pagesGenome Size & Organization, & Gene Regulation in ProkaryotesGayathri deviNo ratings yet
- Effects of Neurotransmitters on Neuronal ReceptorsDocument38 pagesEffects of Neurotransmitters on Neuronal ReceptorsShirlee LarsonNo ratings yet
- Learning Outcome 7Document3 pagesLearning Outcome 7Anj DeograciasNo ratings yet
- DRUGS ACTING ON THE CNS-AnestheticsDocument85 pagesDRUGS ACTING ON THE CNS-AnestheticsHenok GirmaNo ratings yet
- Drugs Targets: Nur Mahmudah Medical Faculty of University Muhammadiyah SurakartaDocument31 pagesDrugs Targets: Nur Mahmudah Medical Faculty of University Muhammadiyah SurakartaRiyani SariNo ratings yet
- Cell Communication and TransportDocument65 pagesCell Communication and TransportCecilia MukototsiNo ratings yet
- Mechanism of Drug Action and Drug Targets: Ligand-Gated Ion Channels (Fast Synaptic Signalling)Document32 pagesMechanism of Drug Action and Drug Targets: Ligand-Gated Ion Channels (Fast Synaptic Signalling)PrabhuRhinsonNo ratings yet
- ReceptorsDocument44 pagesReceptorsAbiy AliyeNo ratings yet
- KULPAK Introduction To Pharmacology of CNS Drugs & Drugs DeliveryDocument47 pagesKULPAK Introduction To Pharmacology of CNS Drugs & Drugs DeliveryfaishalNo ratings yet
- Case Week 2Document2 pagesCase Week 2Reta AzkaNo ratings yet
- A Brazilian Furniture Industry Case StudyDocument17 pagesA Brazilian Furniture Industry Case StudyEnrique MabanoNo ratings yet
- Taketo SUZUKIDocument3 pagesTaketo SUZUKIJane DeckerNo ratings yet
- Multiple Linear RegressionDocument30 pagesMultiple Linear RegressionJonesius Eden ManoppoNo ratings yet
- LU4 OverheadsDocument38 pagesLU4 OverheadsVj TjizooNo ratings yet
- Encoder DecoderDocument6 pagesEncoder Decodermarkcelis1No ratings yet
- AmendmentDocument29 pagesAmendmentYuvraj Singh TenguriyaNo ratings yet
- Snorkel: Rapid Training Data Creation With Weak SupervisionDocument17 pagesSnorkel: Rapid Training Data Creation With Weak SupervisionStephane MysonaNo ratings yet
- Distributes Weight EvenlyDocument5 pagesDistributes Weight Evenlykellie borjaNo ratings yet
- Data Science ArticleDocument2 pagesData Science ArticleRamendra KumarNo ratings yet
- Atterberg's Limits Soil Classification - Liquid Limit, Plastic Limit, ShrinkageDocument5 pagesAtterberg's Limits Soil Classification - Liquid Limit, Plastic Limit, Shrinkagetombasingh100% (1)
- MPT Training CentreDocument11 pagesMPT Training CentreGrace PMNo ratings yet
- Common Customer Gateway Product SheetDocument2 pagesCommon Customer Gateway Product SheetNYSE TechnologiesNo ratings yet
- Vasitars PVT Limited - Pipeline RepairsDocument12 pagesVasitars PVT Limited - Pipeline RepairsPavan_yoyo100% (1)
- Senguntha KshatriyaDocument34 pagesSenguntha Kshatriyabogar marabuNo ratings yet
- UPSC EPFO Previous Year Paper 2017 Questions PDFDocument12 pagesUPSC EPFO Previous Year Paper 2017 Questions PDFPraveenNo ratings yet
- NajeebRehman 1505 14145 1/AFN ExamplesDocument47 pagesNajeebRehman 1505 14145 1/AFN ExamplesQazi JunaidNo ratings yet
- Subtraction Strategies That Lead To RegroupingDocument6 pagesSubtraction Strategies That Lead To Regroupingapi-171857844100% (1)
- LEARNING OBJECTIVESpart2Document4 pagesLEARNING OBJECTIVESpart2sere marcNo ratings yet
- Leadership: Dr. Sayedul Islam Sayed MD Resident, Psychiatry (BSMMU)Document34 pagesLeadership: Dr. Sayedul Islam Sayed MD Resident, Psychiatry (BSMMU)Sayedul IslamNo ratings yet
- Front Office Cover Letter No ExperienceDocument5 pagesFront Office Cover Letter No Experiencec2r7z0x9100% (1)
- X-Ray Artifacts: by DR Mangal S MahajanDocument12 pagesX-Ray Artifacts: by DR Mangal S MahajanTsega HagosNo ratings yet