You might also like
- Ijerph 18 11539 v2Document14 pagesIjerph 18 11539 v2Mobolaji Ayowole victorNo ratings yet
- Understanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsFrom EverandUnderstanding Periodontitis: A Comprehensive Guide to Periodontal Disease for Dentists, Dental Hygienists and Dental PatientsNo ratings yet
- Dental Caries StrategiesDocument23 pagesDental Caries StrategiesCarlos Alberto CastañedaNo ratings yet
- Chronic Marginal PeriodontitisDocument21 pagesChronic Marginal PeriodontitisLaslo Mihaela Larisa100% (1)
- The Health of TeethDocument4 pagesThe Health of TeethGeorgiana Argentina DinuNo ratings yet
- Oral Health Equals Total Health A Brief ReviewDocument4 pagesOral Health Equals Total Health A Brief ReviewFadil ObiNo ratings yet
- GerontoDocument13 pagesGerontoCeza CezaaNo ratings yet
- The Silent Danger of Deep Gum DiseaseDocument1 pageThe Silent Danger of Deep Gum DiseaseLudmila BumbacNo ratings yet
- Perio Caries Recommendations01 Oralhealthteam DEC2021 1Document8 pagesPerio Caries Recommendations01 Oralhealthteam DEC2021 1ioana zaineaNo ratings yet
- The Global Burden of Oral Diseases and Risks To orDocument10 pagesThe Global Burden of Oral Diseases and Risks To orViviane GodoiNo ratings yet
- Periodontal Dissease in ChildrenDocument23 pagesPeriodontal Dissease in ChildrenBiswaroop ChandraNo ratings yet
- Covid-19 Impact An Oral Health With A Focus On Temporomandibular Joint DisordersDocument5 pagesCovid-19 Impact An Oral Health With A Focus On Temporomandibular Joint Disordersbotak berjamaahNo ratings yet
- Oral Diseases A Global Public Health ChallengeDocument12 pagesOral Diseases A Global Public Health ChallengeLaura Garcia RincónNo ratings yet
- 22-09-2022-1663824012-6-Impact - Ijranss-5. Ijranss - Periodontics Diseases Types, Symptoms, and Its CausesDocument10 pages22-09-2022-1663824012-6-Impact - Ijranss-5. Ijranss - Periodontics Diseases Types, Symptoms, and Its CausesImpact JournalsNo ratings yet
- Prevalence of Periodontal Disease in Children With Leukemia and ThalassemiaDocument14 pagesPrevalence of Periodontal Disease in Children With Leukemia and ThalassemiaZackNo ratings yet
- Augpen Dental Cme SlidesDocument43 pagesAugpen Dental Cme SlidesSanjay NavaleNo ratings yet
- 7 L0910 - ENG - 4year - VIIISemester - VNicolaiciucDocument16 pages7 L0910 - ENG - 4year - VIIISemester - VNicolaiciucShany SchwarzwaldNo ratings yet
- Pattern and Factors Associated With Utilisation of Dental ServicesDocument13 pagesPattern and Factors Associated With Utilisation of Dental ServicesKaitwa MbuyaNo ratings yet
- Epidemiology of Oral Health Conditions in Older People: OriginalarticleDocument8 pagesEpidemiology of Oral Health Conditions in Older People: OriginalarticleWJNo ratings yet
- Classification of Periodontal Diseases and Conditions 2018Document15 pagesClassification of Periodontal Diseases and Conditions 2018Jean DatorNo ratings yet
- Dental Caries A ReviewDocument7 pagesDental Caries A ReviewAndrei PaşaniucNo ratings yet
- Dental Caries in Geriatric Dentistry - An Update For CliniciansDocument6 pagesDental Caries in Geriatric Dentistry - An Update For CliniciansfebrinaNo ratings yet
- Management of Patient With Hypodontia: Review of Literature and Case ReportDocument16 pagesManagement of Patient With Hypodontia: Review of Literature and Case ReportAnonymous v2aJxfe9RzNo ratings yet
- Decay and Gum DiseaseDocument8 pagesDecay and Gum DiseaseAANo ratings yet
- Diet, Nutrition, and Prevention of Dental DiseaseDocument26 pagesDiet, Nutrition, and Prevention of Dental DiseaseMuhammad Benny SetiyadiNo ratings yet
- Highlights Symptoms of Periodontal DiseaseDocument12 pagesHighlights Symptoms of Periodontal DiseaseTriana Wahyu SaputriNo ratings yet
- Policy and Practice: The Global Burden of Oral Diseases and Risks To Oral HealthDocument9 pagesPolicy and Practice: The Global Burden of Oral Diseases and Risks To Oral HealththiewyNo ratings yet
- Gambaran Pola Kehilangan Gigi Sebagian Pada MasyarakatDocument6 pagesGambaran Pola Kehilangan Gigi Sebagian Pada MasyarakatrahmaNo ratings yet
- Periodontal Disease and Its Prevention, by Traditional and New Avenues (Review)Document3 pagesPeriodontal Disease and Its Prevention, by Traditional and New Avenues (Review)Louis HutahaeanNo ratings yet
- 7 Oral Health of Geriatric People Modified Copy or ReferenceDocument15 pages7 Oral Health of Geriatric People Modified Copy or ReferenceNitya KrishnaNo ratings yet
- Endo Perio LesionsDocument10 pagesEndo Perio LesionsAlin OdorNo ratings yet
- Periodontal DiseasesDocument12 pagesPeriodontal DiseasesdgdNo ratings yet
- Can Plant Materials Be Valuable in The Treatment of Periodontal Diseases - Practical ReviewDocument22 pagesCan Plant Materials Be Valuable in The Treatment of Periodontal Diseases - Practical ReviewFilipe GonçalvesNo ratings yet
- 1 Periodontology 1 2019 - 0Document12 pages1 Periodontology 1 2019 - 0Shany SchwarzwaldNo ratings yet
- Lec2/ Epidemiology of Dental CariesDocument7 pagesLec2/ Epidemiology of Dental Cariesمحمد العراقيNo ratings yet
- Lec2/ Epidemiology of Dental CariesDocument7 pagesLec2/ Epidemiology of Dental Cariesمحمد العراقيNo ratings yet
- Silk 2014Document16 pagesSilk 2014aaNo ratings yet
- WA Unit 2Document5 pagesWA Unit 2Ben ObiNo ratings yet
- Oral Health ProgramDocument6 pagesOral Health ProgramPoohlarica UyNo ratings yet
- Epidemiology of Dental Caries When Structure and Context MatterDocument7 pagesEpidemiology of Dental Caries When Structure and Context MatterHUGO GOUVEIANo ratings yet
- Managing C R in Adults: Aries ISKDocument6 pagesManaging C R in Adults: Aries ISKSOMVIR KUMARNo ratings yet
- Articulo Cientifico 2, MartesDocument7 pagesArticulo Cientifico 2, MartesValeryNo ratings yet
- IMPORTANTE Promoc Educac Salud Adult MayorDocument4 pagesIMPORTANTE Promoc Educac Salud Adult MayorJorge BalzanNo ratings yet
- Dental Caries MSCDocument137 pagesDental Caries MSCNahla OthmanNo ratings yet
- Journal Homepage: - : IntroductionDocument6 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Chapter37 - Prevention of Periodontal - Dis94 PDFDocument13 pagesChapter37 - Prevention of Periodontal - Dis94 PDFDana DanielaNo ratings yet
- Research PaperDocument7 pagesResearch Paperapi-454004347No ratings yet
- Dental DiseaseDocument15 pagesDental Diseasetien280917No ratings yet
- Dental Hygiene and Periodontal DiseaseDocument7 pagesDental Hygiene and Periodontal Diseaseapi-536835901No ratings yet
- J Mcna 2014 08 002Document22 pagesJ Mcna 2014 08 002nazita dinda sekar norNo ratings yet
- Gingival and Periodontal Diseases in Children and AdolescentsDocument4 pagesGingival and Periodontal Diseases in Children and AdolescentsYuniarPratiwyPanjaitanNo ratings yet
- Sugars and Dental CariesDocument3 pagesSugars and Dental CariestessNo ratings yet
- An Ageing Population Poses Dental Challenges: ReviewDocument6 pagesAn Ageing Population Poses Dental Challenges: ReviewCeza CezaaNo ratings yet
- Wong 2017Document24 pagesWong 2017Ngoc MinhNo ratings yet
- Caries DentalDocument9 pagesCaries DentalGaby Araya AlvarezNo ratings yet
- Distribution of Tooth LossDocument7 pagesDistribution of Tooth LossAndrey YegorovykhNo ratings yet
- Dokumen - Tips 4 Epidemiology of Periodontal Diseases 1pptDocument22 pagesDokumen - Tips 4 Epidemiology of Periodontal Diseases 1pptHimanshu GargNo ratings yet
- Oral Cancer: Easy And Simplified Strategies to Cure Oral Cancer Forever : Early Detection, Prevention And TreatmentFrom EverandOral Cancer: Easy And Simplified Strategies to Cure Oral Cancer Forever : Early Detection, Prevention And TreatmentNo ratings yet
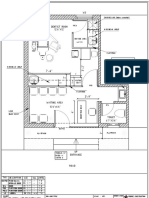
- Dental Clinic - Floor Plan R3-2Document1 pageDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- IPS E-Max ZirCAD LabsideDocument64 pagesIPS E-Max ZirCAD LabsideManuel PutaruNo ratings yet
- Articulo Zadeh Tecnica VISTADocument10 pagesArticulo Zadeh Tecnica VISTApatricia sotoNo ratings yet
- DENT461 - Guided Tissue Regeneration - GTR 2022Document38 pagesDENT461 - Guided Tissue Regeneration - GTR 2022Victoria ChenNo ratings yet
- An Approach To Biomimetics - The Natural CAD - CAM RestorationDocument9 pagesAn Approach To Biomimetics - The Natural CAD - CAM RestorationAngel Rubén Orozco RodríguezNo ratings yet
- Soben Peter Community Dentistry PDFDocument1 pageSoben Peter Community Dentistry PDFyashika guptaNo ratings yet
- NomenclatureDocument12 pagesNomenclatureImran KhanNo ratings yet
- Dental Crowing and Its Relationship To Mesiodistal Crown Diameters and Arch DimensionsDocument7 pagesDental Crowing and Its Relationship To Mesiodistal Crown Diameters and Arch DimensionsMafe SalazarNo ratings yet
- List of Recognised HospitalDocument32 pagesList of Recognised Hospitalgowtham raajNo ratings yet
- Original: Receipt No.Document1 pageOriginal: Receipt No.manjusha rawtiyaNo ratings yet
- Review Questions and Answers For Dental Assisting - Revised Reprint, 2e by Mosby, Betty Ladley Finkbeiner CDA Emeritus BS MSDocument266 pagesReview Questions and Answers For Dental Assisting - Revised Reprint, 2e by Mosby, Betty Ladley Finkbeiner CDA Emeritus BS MSroz nejadiNo ratings yet
- 4 - 3.VV Dental Product CatalogueDocument29 pages4 - 3.VV Dental Product Cataloguedrewyn_19No ratings yet
- UntitledDocument184 pagesUntitledأسامه ممتاز مرادNo ratings yet
- CEO - CaninesDocument17 pagesCEO - CaninesAlina EsanuNo ratings yet
- Cysts of The JawsDocument25 pagesCysts of The Jawsluna zeidNo ratings yet
- Determinacon de La DVO Una Revision Actualizada PDFDocument18 pagesDeterminacon de La DVO Una Revision Actualizada PDFJose Antonio Figuroa AbadoNo ratings yet
- 66 JPR D 20 00116Document13 pages66 JPR D 20 00116AncikNo ratings yet
- Iaad 2023Document4 pagesIaad 2023Swabhaanu SindagiNo ratings yet
- Colgate Optic White Overnight Teeth W PDFDocument2 pagesColgate Optic White Overnight Teeth W PDFMr. HasnatNo ratings yet
- MTA Pulpotomy As An Alternative To Root Canal Treatment in Children's Permanent Teeth in A Dental Public Health Setting.Document6 pagesMTA Pulpotomy As An Alternative To Root Canal Treatment in Children's Permanent Teeth in A Dental Public Health Setting.Abdul Rahman AlmishhdanyNo ratings yet
- DR Pavin Sir ImplantsDocument74 pagesDR Pavin Sir ImplantsAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Place of A New Radiological Index in Predicting Pulp Exposure Before Intervention For Deep Carious LesionsDocument10 pagesPlace of A New Radiological Index in Predicting Pulp Exposure Before Intervention For Deep Carious Lesionssoho1303No ratings yet
- Object Localzation PDFDocument4 pagesObject Localzation PDFMirna MalakNo ratings yet
- Maxicare Dental Hub April 15Document2 pagesMaxicare Dental Hub April 15Va TechIncNo ratings yet
- Gerodontology - Personal Oral Hygiene and Dental Caries A Systematic Review of Randomised ControlledDocument8 pagesGerodontology - Personal Oral Hygiene and Dental Caries A Systematic Review of Randomised Controlledgarnett77No ratings yet
- Temporary Splinting.: Accomplished: Leonte Daniela, S1904Document15 pagesTemporary Splinting.: Accomplished: Leonte Daniela, S1904Daniela LeonteNo ratings yet
- Dental ImplantsDocument1 pageDental Implantsapi-500949236No ratings yet
- Harris1992 The Connective Tissue and Partial Thickness Double Pedicle GraftDocument10 pagesHarris1992 The Connective Tissue and Partial Thickness Double Pedicle GraftAna Maria Montoya GomezNo ratings yet
- Swinglock DentureDocument7 pagesSwinglock DentureLouis HutahaeanNo ratings yet
- Lecture 22 - The Digestive TractDocument32 pagesLecture 22 - The Digestive TractCarl Agape DavisNo ratings yet