You might also like
- Commonly Prescribed Psychotropic MedicationsDocument2 pagesCommonly Prescribed Psychotropic MedicationsDragutin Petrić100% (1)
- IM On Call (LANGE On Call) PDFDocument738 pagesIM On Call (LANGE On Call) PDFindia2puppy100% (8)
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Medication Administration PolicyDocument76 pagesMedication Administration PolicyJully GaciasNo ratings yet
- Antibiotic SlideDocument56 pagesAntibiotic SlidePhongsathorn PhlaisaithongNo ratings yet
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Serum Protein Electrophoresis: Edited by RaniDocument66 pagesSerum Protein Electrophoresis: Edited by RaniMustakim DuharingNo ratings yet
- Antigen and Antibody ReactionDocument43 pagesAntigen and Antibody ReactionSubash SubaNo ratings yet
- MB115 2020 Final Exam 2020Document26 pagesMB115 2020 Final Exam 2020Milimo MweembaNo ratings yet
- Organ SystemsDocument29 pagesOrgan SystemsDonna Remitar100% (2)
- Rheumatoid Arthritis: Andrade, Jhamaica L. Arciaga, Lara Jayne P. Junio, Alyssa MDocument26 pagesRheumatoid Arthritis: Andrade, Jhamaica L. Arciaga, Lara Jayne P. Junio, Alyssa MZofia RanadaNo ratings yet
- Oncology Cheat Sheets - 1Document5 pagesOncology Cheat Sheets - 1abdallahmaurice94No ratings yet
- Rheumatoid ArthritisDocument42 pagesRheumatoid ArthritisNoman MunirNo ratings yet
- 2020 Drugs On Pain (Analgesics) - DENTISTRYDocument28 pages2020 Drugs On Pain (Analgesics) - DENTISTRYVisayan Alliah GailNo ratings yet
- F4) P-Rheumatoid ArthritisDocument11 pagesF4) P-Rheumatoid Arthritisstella.gillesania.chenNo ratings yet
- Antimicrobial Dosage Adjustments in Renal Impairment For FormularyDocument20 pagesAntimicrobial Dosage Adjustments in Renal Impairment For Formularyangkatanjuli2019No ratings yet
- 61.drugs For Inflammatory Bowel DiseaseDocument7 pages61.drugs For Inflammatory Bowel DiseaseireneNo ratings yet
- Tiratam Medical Training (Must To Know 2018Document38 pagesTiratam Medical Training (Must To Know 2018Peter KaiserNo ratings yet
- Management of TB-HIV Co-InfectionDocument17 pagesManagement of TB-HIV Co-InfectionStefanus Raditya PurbaNo ratings yet
- Kemot Erap IDocument27 pagesKemot Erap IHalf BastardNo ratings yet
- Terapi Sistemik Pada Kanker Dengan Obat Anti Kanker (OAK) Pada Saat Pandemi COVID-19Document31 pagesTerapi Sistemik Pada Kanker Dengan Obat Anti Kanker (OAK) Pada Saat Pandemi COVID-19dayarni buuloloNo ratings yet
- Crohns Disease FinalDocument3 pagesCrohns Disease Finalapi-535481376No ratings yet
- OAB113511Document1 pageOAB113511trillion5No ratings yet
- MS FTT S2 2019 PDFDocument37 pagesMS FTT S2 2019 PDFVannyNo ratings yet
- Adult Sepsis Order SetDocument3 pagesAdult Sepsis Order SetYoussef MokdadNo ratings yet
- Antidepressants Anticholinesterases Myestheania GravisDocument16 pagesAntidepressants Anticholinesterases Myestheania GravisShreeNo ratings yet
- Thrombolytic TherapyDocument16 pagesThrombolytic TherapyAnonymous nrZXFwNo ratings yet
- (Terjemahan) Farmakologi Obat Pada Reaksi HipersensitivitasDocument59 pages(Terjemahan) Farmakologi Obat Pada Reaksi HipersensitivitasM Rasya SanimanNo ratings yet
- Reteplase (MIRel)Document23 pagesReteplase (MIRel)Jhoann JamanilaNo ratings yet
- MedicationsDocument63 pagesMedicationssaraNo ratings yet
- Cardiology Doses: WhiteknightloveDocument3 pagesCardiology Doses: WhiteknightloveSelim TarekNo ratings yet
- Management of Rheumatoid ArthritisDocument48 pagesManagement of Rheumatoid ArthritisAlexNo ratings yet
- VTE - Prophylaxis - PROTOCOL - V1.1 - With Forms - 07 - Dec - 2023Document20 pagesVTE - Prophylaxis - PROTOCOL - V1.1 - With Forms - 07 - Dec - 2023hatem newishyNo ratings yet
- VTE Prophylaxis PROTOCOL V1.2 Withforms 31 Dec 2023Document19 pagesVTE Prophylaxis PROTOCOL V1.2 Withforms 31 Dec 2023hatem newishyNo ratings yet
- Emtiaz Guide Internal MD PDFDocument142 pagesEmtiaz Guide Internal MD PDFhumanNo ratings yet
- Mosby - Mosby's Drug Reference For Health Professions, 4e-Mosby (2013) - DeletedDocument3 pagesMosby - Mosby's Drug Reference For Health Professions, 4e-Mosby (2013) - DeletedehsanNo ratings yet
- Management of A Case of Acute PoisoningDocument36 pagesManagement of A Case of Acute PoisoningIndranil KhanNo ratings yet
- Anti-Depressant: Mohd Fikry Bin Mohamad Tahir (Student)Document19 pagesAnti-Depressant: Mohd Fikry Bin Mohamad Tahir (Student)fahmiNo ratings yet
- Nausea and Vomiting Nausea and VomitingDocument6 pagesNausea and Vomiting Nausea and VomitingTHERESA CLAIRE ENCINARESNo ratings yet
- Anti-Tuberculosis DrugsDocument12 pagesAnti-Tuberculosis DrugsAkashNo ratings yet
- Clinical Learning Session-Acute Coronary Syndromes Acs - 1Document31 pagesClinical Learning Session-Acute Coronary Syndromes Acs - 1api-611918048No ratings yet
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- Myocardial Infarction: Dept. of Pharmacology, GMC Amritsar 1Document11 pagesMyocardial Infarction: Dept. of Pharmacology, GMC Amritsar 1Robert KatusabeNo ratings yet
- Perioperative Management Guideline Summary 2022Document3 pagesPerioperative Management Guideline Summary 2022adri20121989No ratings yet
- Pediatric Hospital-Acquired and Ventilator-Associated Pneumonia Topic DiscussionDocument5 pagesPediatric Hospital-Acquired and Ventilator-Associated Pneumonia Topic Discussionapi-602288180No ratings yet
- Medication Research Card SampleDocument1 pageMedication Research Card SamplekennybooboooNo ratings yet
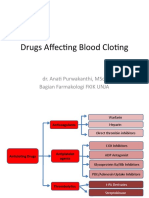
- Drugs Affecting Blood Cloting 2019Document39 pagesDrugs Affecting Blood Cloting 2019Mutiara RizkiNo ratings yet
- MC AtorvastatinDocument3 pagesMC AtorvastatinCliff by the seaNo ratings yet
- Fibrinolytics, Anti Fibrinolytics and Anti Platelets: Dr. B.K.Bezbaruah Professor Pharmacology Gauhati Medical CollegeDocument46 pagesFibrinolytics, Anti Fibrinolytics and Anti Platelets: Dr. B.K.Bezbaruah Professor Pharmacology Gauhati Medical CollegeBidyut BanerjeeNo ratings yet
- 21 by 12 DtyasvydasDocument10 pages21 by 12 DtyasvydasCadR 1No ratings yet
- Lung Cancer Treatment Regimens (Part 1 of 4)Document4 pagesLung Cancer Treatment Regimens (Part 1 of 4)Rubana Reaz TanaNo ratings yet
- Medication Fact Sheets: 3rd Edition ContributorsDocument50 pagesMedication Fact Sheets: 3rd Edition ContributorsIndumathi ThangathirupathiNo ratings yet
- Anti ArrhythmicsDocument46 pagesAnti Arrhythmicsnk999999No ratings yet
- Neuromusculr Blocking Drugs&Reversal Agents and Courses of Delayed RecoveryDocument44 pagesNeuromusculr Blocking Drugs&Reversal Agents and Courses of Delayed RecoverysanjibNo ratings yet
- Drug StudyDocument12 pagesDrug StudySherma Sheikh karimNo ratings yet
- LYRICE ProtocolDocument6 pagesLYRICE ProtocolInas UthmanNo ratings yet
- Venous Thromboembolism With Blanks ResidentsDocument9 pagesVenous Thromboembolism With Blanks Residentsapi-648714317No ratings yet
- Anti Tuberculosis Drugs-1Document26 pagesAnti Tuberculosis Drugs-1bokatiNo ratings yet
- Anti Microbials (Repaired)Document79 pagesAnti Microbials (Repaired)drsidra.mustafaNo ratings yet
- Anti TuberculousDocument45 pagesAnti Tuberculousputri mawarNo ratings yet
- Prinsip AntibiotikDocument33 pagesPrinsip AntibiotikSisisNo ratings yet
- Frontiers in Clinical Drug Research - Anti-Cancer Agents: Volume 5From EverandFrontiers in Clinical Drug Research - Anti-Cancer Agents: Volume 5No ratings yet
- (Transes) Human Histology - 12 Peripheral BloodDocument5 pages(Transes) Human Histology - 12 Peripheral BloodReina CastronuevoNo ratings yet
- Herbal Products Manufacturer Lamina Research CenterDocument30 pagesHerbal Products Manufacturer Lamina Research CenterLamina Research centerNo ratings yet
- Hematology Board ReviewDocument22 pagesHematology Board ReviewEdwin OkonNo ratings yet
- There Are 2 Types of Immunity Active Immunity Passive ImmunityDocument35 pagesThere Are 2 Types of Immunity Active Immunity Passive ImmunityDewi SallehNo ratings yet
- Microbiology SyllabusDocument5 pagesMicrobiology SyllabushhgNo ratings yet
- Full Download Book Endodontics E Book Principles and Practice PDFDocument41 pagesFull Download Book Endodontics E Book Principles and Practice PDFlouis.grant435100% (14)
- Minor Blood Group Notes PDFDocument4 pagesMinor Blood Group Notes PDFChino Paolo SamsonNo ratings yet
- Immunology Made Simple AF FinalDocument77 pagesImmunology Made Simple AF FinalStudy EverydayNo ratings yet
- Disease and ImmunityDocument22 pagesDisease and ImmunityGuna VallabhNo ratings yet
- Practical Answers DCPIPDocument98 pagesPractical Answers DCPIPSanad BashirNo ratings yet
- Biotechnology: Quarter 2 - Module 4-5 Week 4-5 - Biotechnology and HealthDocument31 pagesBiotechnology: Quarter 2 - Module 4-5 Week 4-5 - Biotechnology and HealthSheena Mae A. ComingNo ratings yet
- 4-Cell Mediated ImmunityDocument34 pages4-Cell Mediated ImmunityleeminhoangrybirdNo ratings yet
- APCH1 - Single Chain Antibody For Vaccine TargetingDocument6 pagesAPCH1 - Single Chain Antibody For Vaccine TargetingAgustín OstachukNo ratings yet
- MCAT Content Outline TrackerDocument83 pagesMCAT Content Outline TrackerNoelani-Mei AscioNo ratings yet
- Mohit CBC 18Document1 pageMohit CBC 18amit2352842No ratings yet
- Hematopoiesis ErythropoiesisDocument8 pagesHematopoiesis ErythropoiesisASHLEY ALEXIS GUEVARRANo ratings yet
- I Putu Dedy ArjitoDocument119 pagesI Putu Dedy ArjitoIrfan NugrahaNo ratings yet
- A New Generation of Artificial Enzymes: Catalytic Antibodies or Abzymes'Document30 pagesA New Generation of Artificial Enzymes: Catalytic Antibodies or Abzymes'Arshia KohliNo ratings yet
- AntigensDocument25 pagesAntigensEssington BeloNo ratings yet
- ZB0076 (Bahasa Inggris)Document4 pagesZB0076 (Bahasa Inggris)Hendra BaktiNo ratings yet
- Eji 201847659Document7 pagesEji 201847659marjoranovaNo ratings yet
- SANOFI Brochure Partnering 2019 en PDF e Accessible 01Document31 pagesSANOFI Brochure Partnering 2019 en PDF e Accessible 01Vianney Casta¥Eda MonroyNo ratings yet
- Erba Mannheim - Basic Immunology Training - Version 1.1Document35 pagesErba Mannheim - Basic Immunology Training - Version 1.1Arnoldo FelixNo ratings yet
- HES 032 BSN - Lecture Long Quiz 3 FINALDocument24 pagesHES 032 BSN - Lecture Long Quiz 3 FINALGem HimenaceNo ratings yet
- Hasil Pemeriksaan Rapid Antibody Peserta KarantinaDocument22 pagesHasil Pemeriksaan Rapid Antibody Peserta Karantinac10101herikurniawanNo ratings yet
- ISlabDocument3 pagesISlabpixiedustNo ratings yet