You might also like
- Textbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationFrom EverandTextbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationNo ratings yet
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsFrom EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsNo ratings yet
- Unit 1 Documentation-and-ReportingDocument39 pagesUnit 1 Documentation-and-ReportingMs.V. Mahesha Asst. Prof.No ratings yet
- Documentation in Nursing: Mahmood AhmedDocument41 pagesDocumentation in Nursing: Mahmood Ahmedjoan olanteNo ratings yet
- Legal Protection of Nursing ServiceDocument4 pagesLegal Protection of Nursing ServiceJanna Kristine Ferrer Yosores80% (5)
- Documentation in NursingDocument43 pagesDocumentation in NursingMAHMOOD AHMED100% (19)
- Records and ReportDocument4 pagesRecords and ReportAnusikta PandaNo ratings yet
- and Report Fy BSC FonDocument43 pagesand Report Fy BSC FonNainesh soyantarNo ratings yet
- CN - Day 2Document117 pagesCN - Day 24k4ghcxfv2No ratings yet
- 9 3 2012 Charting and DocumentationDocument44 pages9 3 2012 Charting and DocumentationMacrossBalaNo ratings yet
- 1.1 Background Nursing Documentation Is The Record of Nursing Care That Is Planned and Delivered ToDocument13 pages1.1 Background Nursing Documentation Is The Record of Nursing Care That Is Planned and Delivered Toari cendani prabawatiNo ratings yet
- NICU Documentation: Gama Hospital Al Khobar K.S.ADocument8 pagesNICU Documentation: Gama Hospital Al Khobar K.S.ALucian CaelumNo ratings yet
- Nursing Report What You Need To Include When Writing A Nursing ReportDocument2 pagesNursing Report What You Need To Include When Writing A Nursing ReportAnnisa Nurul SafitriNo ratings yet
- 14. Nursing DocumentationDocument58 pages14. Nursing Documentationhassanburhan27No ratings yet
- Documentation and ReportingDocument17 pagesDocumentation and Reportingsonam MaclayNo ratings yet
- Documentation in NursingDocument41 pagesDocumentation in NursingGLAIZA PALATINONo ratings yet
- Documentation and ReportingDocument71 pagesDocumentation and ReportingnamNo ratings yet
- Recording and reporting in hospitals and nursing collegesDocument48 pagesRecording and reporting in hospitals and nursing collegesRaja100% (2)
- Week 13 Documentation in Psychiatric Mental Health Nursing PracticeDocument69 pagesWeek 13 Documentation in Psychiatric Mental Health Nursing PracticeJeff MalinisNo ratings yet
- Records and Reports-AnuDocument89 pagesRecords and Reports-AnuNithiya NadesanNo ratings yet
- Documentation: Basic Nursing: Foundations of Skills & Concepts DocumentationDocument8 pagesDocumentation: Basic Nursing: Foundations of Skills & Concepts DocumentationJona GarzonNo ratings yet
- Documentation 1Document26 pagesDocumentation 1WaaberrinNo ratings yet
- Maintenance of Documentation NVQ 6Document32 pagesMaintenance of Documentation NVQ 6samitha madurangaNo ratings yet
- Focus Charting at North Bay General Hospital DAEDocument67 pagesFocus Charting at North Bay General Hospital DAECzarina GuintoNo ratings yet
- DOCUMENTATIONDocument84 pagesDOCUMENTATIONTrisha Mae BalladNo ratings yet
- Documentation 2016Document52 pagesDocumentation 2016jenNo ratings yet
- Documentation Documentation of Patient Teaching Characteristics of Documentation Components of DocumentationDocument10 pagesDocumentation Documentation of Patient Teaching Characteristics of Documentation Components of DocumentationLira MacoNo ratings yet
- Maintenance of Records and ReportsDocument81 pagesMaintenance of Records and ReportsSanjna Kumari (SNSR Senior Tutor/Lecturer)100% (1)
- 151nursingdocumentation PDFDocument24 pages151nursingdocumentation PDFpademenNo ratings yet
- Documentation System Focus ChartingDocument26 pagesDocumentation System Focus ChartingneehoshiNo ratings yet
- Documenting, Reporting, Conferring, and Using InformaticsDocument92 pagesDocumenting, Reporting, Conferring, and Using InformaticsZhiela Esteban AbivaNo ratings yet
- Cmca Rle L1 DocumentationDocument23 pagesCmca Rle L1 DocumentationJay EstrellaNo ratings yet
- CHARTING BASICS GUIDEDocument11 pagesCHARTING BASICS GUIDEfarahdlc100% (1)
- Steve M. Esteban RN, LPT, MSN, ManDocument39 pagesSteve M. Esteban RN, LPT, MSN, ManSteve EstebanNo ratings yet
- Nursing Documentation and ReportingDocument0 pagesNursing Documentation and ReportingJames Avoka Asamani83% (6)
- Documentation: Written Evidence ofDocument30 pagesDocumentation: Written Evidence ofAnggraeni Prameswari PutriNo ratings yet
- 2015 DocumentationDocument25 pages2015 Documentationdext9355No ratings yet
- Nursing RecordsDocument20 pagesNursing Recordstessy mathewNo ratings yet
- Nursing Record and ReportsDocument32 pagesNursing Record and ReportsOm VaishNav100% (1)
- Nursing DocumentationDocument17 pagesNursing Documentationprema100% (4)
- Nursing DiagnosisDocument38 pagesNursing DiagnosisJR Rolf NeuqeletNo ratings yet
- Group11 MOPDocument5 pagesGroup11 MOPjilliantrcieNo ratings yet
- Documentation and SBARDocument25 pagesDocumentation and SBARmahmoud ShakriaNo ratings yet
- NapulanRM - Health Records Analysis and Clinical AuditDocument64 pagesNapulanRM - Health Records Analysis and Clinical AuditJeffreyReyesNo ratings yet
- Chapter 26Document46 pagesChapter 26meeeenonNo ratings yet
- Nursing Process and Documentation GuideDocument52 pagesNursing Process and Documentation Guidegeorgeloto12100% (2)
- Relevance of Nursing Documentation and Its Legal ImplicationsDocument8 pagesRelevance of Nursing Documentation and Its Legal ImplicationsGeorge AyiteyNo ratings yet
- Specific Skills: Types of Documentation: 1. RecordingDocument5 pagesSpecific Skills: Types of Documentation: 1. Recordingmsah820No ratings yet
- Midterms - HA LabDocument17 pagesMidterms - HA LabMa. Daniela De la CernaNo ratings yet
- Nursing Documentation1Document3 pagesNursing Documentation1Paskuman DinkesNo ratings yet
- Skills in Documenting and ReportingDocument9 pagesSkills in Documenting and ReportingcjNo ratings yet
- Documenting and ReportingDocument5 pagesDocumenting and ReportingElla LobenariaNo ratings yet
- DocumentationandreportingDocument43 pagesDocumentationandreportingharley dela cruzNo ratings yet
- Nursing ProcessDocument52 pagesNursing ProcessDzon LornaNo ratings yet
- Document It RightDocument61 pagesDocument It RightMacrossBala100% (1)
- Medical Records Doc GuideDocument51 pagesMedical Records Doc Guidealwy aliNo ratings yet
- NCM-101 - Module-7 - 2Document39 pagesNCM-101 - Module-7 - 2Princess Javier TorcelinoNo ratings yet
- Teaching Learning Activities (TLA)Document10 pagesTeaching Learning Activities (TLA)Kristil ChavezNo ratings yet
- 151 Nursing DocumentationDocument24 pages151 Nursing DocumentationNasrullah UllahNo ratings yet
- Newman's Certified Electronic Health Records Technician Study GuideFrom EverandNewman's Certified Electronic Health Records Technician Study GuideNo ratings yet
- CURRICULUM AUDIT: GRADE 7 MATHEMATICSDocument5 pagesCURRICULUM AUDIT: GRADE 7 MATHEMATICSjohnalcuinNo ratings yet
- The Interview: P F T IDocument14 pagesThe Interview: P F T IkkkkccccNo ratings yet
- Bal - 2011 - The New HRM in The 21st Century - A Strategic ViewDocument15 pagesBal - 2011 - The New HRM in The 21st Century - A Strategic ViewJoaquínMartínezMiñoNo ratings yet
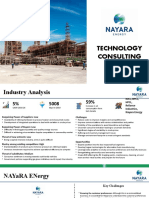
- Technology Consulting: Amruta Kulkarni Anu Abraham Rajat JainDocument9 pagesTechnology Consulting: Amruta Kulkarni Anu Abraham Rajat JainRajat JainNo ratings yet
- IPO Fact Sheet - Accordia Golf Trust 140723Document4 pagesIPO Fact Sheet - Accordia Golf Trust 140723Invest StockNo ratings yet
- Admission Procedure For International StudentsDocument8 pagesAdmission Procedure For International StudentsAndreea Anghel-DissanayakaNo ratings yet
- District Wise List of Colleges Under The Juridiction of MRSPTU BathindaDocument13 pagesDistrict Wise List of Colleges Under The Juridiction of MRSPTU BathindaGurpreet SandhuNo ratings yet
- Variables in Language Teaching - The Role of The TeacherDocument34 pagesVariables in Language Teaching - The Role of The TeacherFatin AqilahNo ratings yet
- Airs-Lms - Math-10 - q3 - Week 3-4 Module 3 Rhonavi MasangkayDocument19 pagesAirs-Lms - Math-10 - q3 - Week 3-4 Module 3 Rhonavi MasangkayRamil J. Merculio100% (1)
- One - Pager - SOGEVAC SV 320 BDocument2 pagesOne - Pager - SOGEVAC SV 320 BEOLOS COMPRESSORS LTDNo ratings yet
- PediculosisDocument14 pagesPediculosisREYMARK HACOSTA100% (1)
- Lineapelle: Leather & Non-LeatherDocument16 pagesLineapelle: Leather & Non-LeatherShikha BhartiNo ratings yet
- Strategic Flexibility: The Evolving Paradigm of Strategic ManagementDocument3 pagesStrategic Flexibility: The Evolving Paradigm of Strategic Managementnanthini kanasanNo ratings yet
- Oracle Apps Quality ModuleDocument17 pagesOracle Apps Quality ModuleSantOsh100% (2)
- Mad LabDocument66 pagesMad LabBalamurugan MNo ratings yet
- Maths SolutionDocument10 pagesMaths SolutionAbhay KumarNo ratings yet
- Project Report Software and Web Development Company: WWW - Dparksolutions.inDocument12 pagesProject Report Software and Web Development Company: WWW - Dparksolutions.inRavi Kiran Rajbhure100% (1)
- Circuit AnalysisDocument98 pagesCircuit Analysisahtisham shahNo ratings yet
- Oracle® E-Business Suite: Integrated SOA Gateway Implementation Guide Release 12.2Document202 pagesOracle® E-Business Suite: Integrated SOA Gateway Implementation Guide Release 12.2yadavdevenderNo ratings yet
- Oracle Unified Method (OUM) White Paper - Oracle's Full Lifecycle Method For Deploying Oracle-Based Business Solutions - GeneralDocument17 pagesOracle Unified Method (OUM) White Paper - Oracle's Full Lifecycle Method For Deploying Oracle-Based Business Solutions - GeneralAndreea Mirosnicencu100% (1)
- Lateral capacity of pile in clayDocument10 pagesLateral capacity of pile in clayGeetha MaNo ratings yet
- Why Islam Is The True Religion in Light of The Quran and SunnahDocument7 pagesWhy Islam Is The True Religion in Light of The Quran and SunnahAsmau DaboNo ratings yet
- Presentation 1Document20 pagesPresentation 1nikitakhanduja1304No ratings yet
- 16 Week Mountain Marathon Training Plan: WWW - Brutalevents.co - UkDocument2 pages16 Week Mountain Marathon Training Plan: WWW - Brutalevents.co - UkCristina CrsNo ratings yet
- Political Engineering and Party Politics in Conflict-Prone SocietiesDocument18 pagesPolitical Engineering and Party Politics in Conflict-Prone SocietiesNashiba Dida-AgunNo ratings yet
- British Isles Composition GuideDocument4 pagesBritish Isles Composition GuidesonmatanalizNo ratings yet
- A Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulDocument19 pagesA Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulweetrydhNo ratings yet
- Aerospace Opportunities in SwitzerlandDocument5 pagesAerospace Opportunities in SwitzerlandBojana DekicNo ratings yet
- CHEMICAL ANALYSIS OF WATER SAMPLEDocument5 pagesCHEMICAL ANALYSIS OF WATER SAMPLEAiron Fuentes EresNo ratings yet
- The Unbounded MindDocument190 pagesThe Unbounded MindXtof ErNo ratings yet