You might also like
- Ophthalmology PDFDocument28 pagesOphthalmology PDFKukuh Rizwido PrasetyoNo ratings yet
- Clinical Ophthalmology for UndergraduatesFrom EverandClinical Ophthalmology for UndergraduatesRating: 4 out of 5 stars4/5 (5)
- Parasitology TablesDocument9 pagesParasitology Tables2013SecB92% (26)
- Retinal DetachmentDocument31 pagesRetinal DetachmentEko KunaryagiNo ratings yet
- Cataract And Small Pupil Management Manual Techniques: 2022, #1From EverandCataract And Small Pupil Management Manual Techniques: 2022, #1No ratings yet
- Ocular EmergenciesDocument26 pagesOcular EmergenciesYukianesa100% (1)
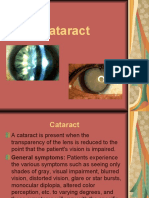
- CataractDocument3 pagesCataractShereen ManabilangNo ratings yet
- Disorders of Skin in ChildrenDocument47 pagesDisorders of Skin in Childrensmriti boraNo ratings yet
- Glaucoma and CataractDocument30 pagesGlaucoma and CataractJayselle ArvieNo ratings yet
- Nclex EyesDocument9 pagesNclex EyesYoke W Khoo100% (1)
- Cataract PPT FinalDocument37 pagesCataract PPT FinalSibi John91% (22)
- Anatomy of Human EyeDocument41 pagesAnatomy of Human EyeCarly MelachioNo ratings yet
- Common Ocular EmergenciesDocument33 pagesCommon Ocular EmergenciesMaimoona AimanNo ratings yet
- Case Study Part 2 Patient With Uti (Bag-O)Document48 pagesCase Study Part 2 Patient With Uti (Bag-O)Eaht Quirong0% (1)
- Nephrotic SyndromeDocument23 pagesNephrotic SyndromeamlymarsNo ratings yet
- Ophthalmology - Systemic - Community OphthalmologyDocument7 pagesOphthalmology - Systemic - Community OphthalmologyjbtcmdtjjvNo ratings yet
- Diskusi Topik - Ali Mustagi - Mata Normal Visus Turun PerlahanDocument73 pagesDiskusi Topik - Ali Mustagi - Mata Normal Visus Turun PerlahanalimustagialgiNo ratings yet
- Acquired CataractDocument40 pagesAcquired Cataractapi-3742497No ratings yet
- Phatology The Eyelids, Lacrimal GlandsDocument62 pagesPhatology The Eyelids, Lacrimal GlandsGermanyNo ratings yet
- PHLYCTENULAR ConjunctivitsDocument17 pagesPHLYCTENULAR Conjunctivitsapi-3742497100% (1)
- Ophthalmology - Diseases of VitreousDocument5 pagesOphthalmology - Diseases of VitreousjbtcmdtjjvNo ratings yet
- Abnormalities of EyeDocument74 pagesAbnormalities of EyeHikmat UllahNo ratings yet
- Normal Eyes With Gradually Decrease VisionDocument73 pagesNormal Eyes With Gradually Decrease VisionGustiAngriAngalanNo ratings yet
- Jewel June Gutierrez N-31 Rosejel Mae Lagura Senile Cataract IDocument4 pagesJewel June Gutierrez N-31 Rosejel Mae Lagura Senile Cataract IJewel GutierrezNo ratings yet
- Retinal DetachmentDocument3 pagesRetinal DetachmentRownald Lakandula PanuncialNo ratings yet
- Diseases of The Eyelids: Mshangila Barnabas MD, M.MedDocument31 pagesDiseases of The Eyelids: Mshangila Barnabas MD, M.MedCharles AnthonyNo ratings yet
- Ent Lesson 8Document45 pagesEnt Lesson 8favourednancie9No ratings yet
- Cataract: Deasy Mirayashi (I11110003)Document46 pagesCataract: Deasy Mirayashi (I11110003)Yunia DwiNo ratings yet
- Retinaldetachmentnew WORSDocument51 pagesRetinaldetachmentnew WORSMuthulakshmiNo ratings yet
- Disease of Orbit, LacrimalDocument73 pagesDisease of Orbit, LacrimalMarshet GeteNo ratings yet
- Five Year PROSE Treatment For Aniridic KojimaOct2016PAPDocument5 pagesFive Year PROSE Treatment For Aniridic KojimaOct2016PAP小島隆司No ratings yet
- Trauma MataDocument57 pagesTrauma MataFatmala Umi MaisarahNo ratings yet
- English Premium Exam: Filial de Ciencias Médicas of BaracoaDocument9 pagesEnglish Premium Exam: Filial de Ciencias Médicas of BaracoaDouglas Soslan Reyes FiffeNo ratings yet
- Emailing Ophthalmology - Past Papers SEQS - KMUDocument70 pagesEmailing Ophthalmology - Past Papers SEQS - KMUem khan100% (2)
- Introduction, Health History, GordonsDocument10 pagesIntroduction, Health History, GordonsKayelyn-Rose CombateNo ratings yet
- Kelenjar LakrimalDocument44 pagesKelenjar LakrimalNurfanida Natasya MNo ratings yet
- Retinal DetachmentDocument21 pagesRetinal DetachmentRose O'SullivanNo ratings yet
- Current Trend in Medical Treatment of Dry Eye SyndromeDocument43 pagesCurrent Trend in Medical Treatment of Dry Eye SyndromeFaiz NazriNo ratings yet
- 2019 Dr. Sahilah PalpebraDocument31 pages2019 Dr. Sahilah PalpebraDEWI MULYANINo ratings yet
- Eyelid Disorders - Diagnosis and Management - AAFPDocument15 pagesEyelid Disorders - Diagnosis and Management - AAFPMufassiraturrahmahNo ratings yet
- Corneal DegenerationDocument1 pageCorneal Degenerationtgrrwccj98No ratings yet
- Retinal Detachment Is A Disorder of The Eye in Which The Retina Peels Away From Its Underlying Layer of Support TissueDocument5 pagesRetinal Detachment Is A Disorder of The Eye in Which The Retina Peels Away From Its Underlying Layer of Support TissuejobinbionicNo ratings yet
- Summary OphthalmologyDocument86 pagesSummary Ophthalmologymarina_shawkyNo ratings yet
- Eyelids AdnexalDocument52 pagesEyelids AdnexalRushdaNo ratings yet
- CBL Week 10Document5 pagesCBL Week 10Sarah ZaheerNo ratings yet
- Penyakit Palpebra Dan AdneksaDocument39 pagesPenyakit Palpebra Dan AdneksaayucicuNo ratings yet
- BY: Achin Pant 3 Year MbbsDocument59 pagesBY: Achin Pant 3 Year MbbsMitali MohanNo ratings yet
- Casos Clínicos Sobre UveíteDocument16 pagesCasos Clínicos Sobre UveíteMirella Lopes da RochaNo ratings yet
- Activity5 (Retinal Detachment)Document3 pagesActivity5 (Retinal Detachment)Gabbii CincoNo ratings yet
- IBKV2 UAS Notes 2022Document24 pagesIBKV2 UAS Notes 2022Anna TohNo ratings yet
- GLAUCOMA (Compatibility Mode)Document17 pagesGLAUCOMA (Compatibility Mode)Ritesh SoodNo ratings yet
- Retinal Detachment and HomoeopathyDocument7 pagesRetinal Detachment and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Diseases of Eyelid: Prepared by DR - Sourab Kumar DasDocument66 pagesDiseases of Eyelid: Prepared by DR - Sourab Kumar Dasসপ্নে ছোয়া মনNo ratings yet
- Assessment of The EYESDocument64 pagesAssessment of The EYESAlliah Marie CababarosNo ratings yet
- Laser-Assisted in Situ KeratomileusisDocument3 pagesLaser-Assisted in Situ KeratomileusisJoe RealNo ratings yet
- Сataract 09Document32 pagesСataract 09somebody_maNo ratings yet
- LENS INDUCED GLAUCOMA - FinallyDocument58 pagesLENS INDUCED GLAUCOMA - FinallySriniwasNo ratings yet
- Cataract Not FixedDocument41 pagesCataract Not FixedDeasy MirayashiNo ratings yet
- Primary Retinal Detachment: Clinical PracticeDocument9 pagesPrimary Retinal Detachment: Clinical PracticeAdita DitaNo ratings yet
- Cataract: Antony Halim I4061162030Document50 pagesCataract: Antony Halim I4061162030Gilang PramanayudhaNo ratings yet
- Opthalmology CasesDocument10 pagesOpthalmology CasesAhmad SobihNo ratings yet
- 15.ocular ProsthesisDocument156 pages15.ocular ProsthesisrajaniNo ratings yet
- Dr. Dr. Habibah S. Muhiddin, SP.M (K) : Departement of Ophthalmology Faculty of Medicine Hasanuddin UniversityDocument31 pagesDr. Dr. Habibah S. Muhiddin, SP.M (K) : Departement of Ophthalmology Faculty of Medicine Hasanuddin UniversityRey AlwiwikhNo ratings yet
- Complicationts of Cataract Surgery (Other Anterior Segment Complications)Document30 pagesComplicationts of Cataract Surgery (Other Anterior Segment Complications)Hikban FiqhiNo ratings yet
- Developmental CatDocument27 pagesDevelopmental Catapi-3742497No ratings yet
- Lens IntroductionDocument40 pagesLens Introductionapi-3756649100% (1)
- Treatment GuidelinesDocument40 pagesTreatment Guidelinesapi-3742497No ratings yet
- Paralytic SquintDocument3 pagesParalytic Squintapi-3756649100% (2)
- AphakiaDocument26 pagesAphakiaapi-3742497100% (3)
- Management of CataractDocument25 pagesManagement of Cataractapi-3742497No ratings yet
- Congenital CataractDocument49 pagesCongenital Cataractapi-3742497100% (2)
- Vernal Keratoconjunctivitis (VKC)Document19 pagesVernal Keratoconjunctivitis (VKC)api-3742497No ratings yet
- Diseasesof ConjunctivaDocument86 pagesDiseasesof Conjunctivaapi-3742497No ratings yet
- Proposal For Up-GradationDocument21 pagesProposal For Up-Gradationapi-3742497No ratings yet
- TRACHOMADocument50 pagesTRACHOMAapi-3742497100% (2)
- Angle Closure Glaucoma - Current ConceptsDocument77 pagesAngle Closure Glaucoma - Current Conceptsapi-3742497100% (3)
- MORNING REPORT Ipd 040914Document22 pagesMORNING REPORT Ipd 040914Teddy PrawiroNo ratings yet
- Small Renal MassDocument26 pagesSmall Renal MassSausan RasmiyyahNo ratings yet
- Nutrition in Kidney Disease Core CurriculumDocument13 pagesNutrition in Kidney Disease Core CurriculumMiguel Ángel DomínguezNo ratings yet
- Diclofenac Induced Paroxysmal Atrial Fibrillation (#536628) - 665053Document3 pagesDiclofenac Induced Paroxysmal Atrial Fibrillation (#536628) - 665053BernadetteLintNo ratings yet
- Frozen SectionDocument9 pagesFrozen SectionBabatunde AjibolaNo ratings yet
- Diagnosa Icd - 10Document2 pagesDiagnosa Icd - 10Yoery SadewoNo ratings yet
- Achilles Speedbridge Repair Implant System: Surgical TechniqueDocument8 pagesAchilles Speedbridge Repair Implant System: Surgical TechniqueSusan Ly VillalobosNo ratings yet
- Placenta AbruptionDocument86 pagesPlacenta AbruptionXena IngalNo ratings yet
- Faq: Un System-Wide Covid-19 Vaccination ProgrammeDocument22 pagesFaq: Un System-Wide Covid-19 Vaccination ProgrammelelloNo ratings yet
- Chiropractic Principles:: Ancient Foundations of Manual Medicine, Metaphysics and ScienceDocument3 pagesChiropractic Principles:: Ancient Foundations of Manual Medicine, Metaphysics and Scienceapi-301357653No ratings yet
- Assissting FNAB in The Liver Liver Biopsy Checklist FinalDocument10 pagesAssissting FNAB in The Liver Liver Biopsy Checklist FinalCamille T. SanchezNo ratings yet
- Carrageenan 1Document4 pagesCarrageenan 1Cao Đức Duy (19140345)No ratings yet
- No Nama Obat Ven Sediaan Harga SatuanjumlahDocument2 pagesNo Nama Obat Ven Sediaan Harga SatuanjumlahCINDYAH ANASTASIA CLARITANo ratings yet
- Beckwith-Wiedemann SyndromeDocument2 pagesBeckwith-Wiedemann Syndromeapi-19976646No ratings yet
- Calcium Channel BlockersDocument28 pagesCalcium Channel Blockershap hazardNo ratings yet
- History Taking in Pulmonary MedicineDocument14 pagesHistory Taking in Pulmonary MedicinestudymedicNo ratings yet
- IMCIDocument17 pagesIMCIapi-3707883No ratings yet
- 300+ TOP CASE MANAGER Objective Questions and AnswersDocument29 pages300+ TOP CASE MANAGER Objective Questions and AnswersHANEESH JOHNNo ratings yet
- NCP MakingDocument2 pagesNCP MakingMinakaNo ratings yet
- WHO Surgical Safety Checklist: Before Induction On AnesthesiaDocument1 pageWHO Surgical Safety Checklist: Before Induction On AnesthesiaDienizs LabiniNo ratings yet
- Clinical Oral Implants Res - 2023 - Schwarz - Effectiveness of Modified and Control Protocols For The Surgical Therapy ofDocument27 pagesClinical Oral Implants Res - 2023 - Schwarz - Effectiveness of Modified and Control Protocols For The Surgical Therapy ofIsaac MoNo ratings yet
- Section A: MCQ (80 Questions)Document16 pagesSection A: MCQ (80 Questions)Muhammed MostafaNo ratings yet
- 4TH QTR ScaffoldDocument1 page4TH QTR ScaffoldGWYNETTE CAMIDCHOLNo ratings yet
- Project On AidsDocument7 pagesProject On AidsRoshanGS20% (5)
- Medical Termination of PregnancyDocument8 pagesMedical Termination of PregnancyNikhil BijuNo ratings yet