You might also like
- Dialogue and Process in Relational Gestalt TherapyDocument3 pagesDialogue and Process in Relational Gestalt Therapysvetiljka50% (2)
- Endocrine Disorders and Their Effects in OrthodonticsDocument29 pagesEndocrine Disorders and Their Effects in OrthodonticsSurabhi SaxenaNo ratings yet
- Bahasa Inggris AskepDocument4 pagesBahasa Inggris AskepMona Indah100% (2)
- Practice of Electroconvulsive Therapy Recommendations For Treatment Training and PrivilDocument364 pagesPractice of Electroconvulsive Therapy Recommendations For Treatment Training and PrivilNícolas AugustoNo ratings yet
- Drugs For Bone Disorders CompleteDocument18 pagesDrugs For Bone Disorders CompleteOmar AbdullahiNo ratings yet
- OsteoporosisDocument24 pagesOsteoporosisMousa SuhailNo ratings yet
- 3 OsteoporosisDocument6 pages3 Osteoporosisiraqeana100100No ratings yet
- Drugs Affecting On Osteoporosis #3Document14 pagesDrugs Affecting On Osteoporosis #3Aryan PandeyNo ratings yet
- Drugs Effecting On Osteoporosis: Abdullaev Dzhumadil, Pharmd International Medical UniversityDocument25 pagesDrugs Effecting On Osteoporosis: Abdullaev Dzhumadil, Pharmd International Medical UniversityRtxGaming Zone 73No ratings yet
- Drugs For OsteoporosisDocument4 pagesDrugs For OsteoporosisJanine Castro SuguitanNo ratings yet
- BisphosphonateDocument33 pagesBisphosphonatelavate amol bhimraoNo ratings yet
- SR 2Document33 pagesSR 2hussein alnasryNo ratings yet
- Rheumatologic Disorders: OsteoporosisDocument7 pagesRheumatologic Disorders: Osteoporosisمحمد رحمان محمد الدليميNo ratings yet
- OP ملونة كاملةDocument27 pagesOP ملونة كاملةArcangela QuaintrelleNo ratings yet
- Kelompok 6 OsteoporosisDocument10 pagesKelompok 6 OsteoporosisNur Indah FitrianaDewiNo ratings yet
- Freeman Hospital, Newcastle Upon Tyne, United KingdomDocument21 pagesFreeman Hospital, Newcastle Upon Tyne, United KingdomcozcozNo ratings yet
- Drugs in OrthopedicsDocument26 pagesDrugs in OrthopedicsRoshandiep GillNo ratings yet
- Bisphosphonates: - Bisphosphonates (Also Called Diphosphonates) Are A Class of Drugs That Prevent The Loss of Bone MassDocument3 pagesBisphosphonates: - Bisphosphonates (Also Called Diphosphonates) Are A Class of Drugs That Prevent The Loss of Bone Massglaire927No ratings yet
- Musculoskeletal DisordersDocument158 pagesMusculoskeletal DisordersJona Kristin EnclunaNo ratings yet
- Non Hormonal AgentsDocument5 pagesNon Hormonal AgentsMarianne CruzNo ratings yet
- Osteoporosis: Dr. Lubna DwerijDocument26 pagesOsteoporosis: Dr. Lubna DwerijNoor MajaliNo ratings yet
- OsteoporosisDocument22 pagesOsteoporosisPrachi DSaNo ratings yet
- Osteoporosis Clinical Case by SlidesgoDocument30 pagesOsteoporosis Clinical Case by SlidesgoHussein Al-jmrawiNo ratings yet
- Osteoporosis, Rickets and OsteomalaciaDocument43 pagesOsteoporosis, Rickets and OsteomalaciahasNo ratings yet
- Osteoporosis: Done By: Dalal Hussain AlanaziDocument15 pagesOsteoporosis: Done By: Dalal Hussain AlanazidallasNo ratings yet
- Medical Management of Osteoporosis in Menopausal WomenDocument11 pagesMedical Management of Osteoporosis in Menopausal WomenSiri DevarapalliNo ratings yet
- OsteoporosisDocument13 pagesOsteoporosisRuaa MalekNo ratings yet
- Presentation On Osteoporosis: Submitted To: Dr. Divya Vohra Submitted By: Sharique Raza M.pharm Jamia HamdardDocument38 pagesPresentation On Osteoporosis: Submitted To: Dr. Divya Vohra Submitted By: Sharique Raza M.pharm Jamia Hamdardsri susantiiNo ratings yet
- Alendronate Study on Bone LossDocument12 pagesAlendronate Study on Bone LossTrio San LuisNo ratings yet
- Masculoskeletal Disorders PharmacotherapyDocument101 pagesMasculoskeletal Disorders PharmacotherapyWaaqoo Guutuu Waaqoo GuutuuNo ratings yet
- BiphosphonatesDocument14 pagesBiphosphonatesadrianajg.drNo ratings yet
- Osteoporosis DR SawsawDocument19 pagesOsteoporosis DR SawsawNariman SternNo ratings yet
- Presented By: Safa Riaz Presented To: Sir Ahmed Watoo Sap Id: 70095869 Topic: OsteoporosisDocument31 pagesPresented By: Safa Riaz Presented To: Sir Ahmed Watoo Sap Id: 70095869 Topic: OsteoporosisSafa RiazNo ratings yet
- Alendronic AcidDocument1 pageAlendronic AcidRPh Krishna Chandra JagritNo ratings yet
- OsteoporosisDocument11 pagesOsteoporosisNisaar Jogi100% (1)
- Osteoporosis Medications Video, Anatomy & Definition OsmosisDocument1 pageOsteoporosis Medications Video, Anatomy & Definition OsmosisLorenaNo ratings yet
- The Dental Implication of Bisphosphonates RJNDocument10 pagesThe Dental Implication of Bisphosphonates RJNmaxfaxNo ratings yet
- Musculoskeletal SystemDocument60 pagesMusculoskeletal Systempetite_chien15No ratings yet
- Long-Term and Sequential Treatment For Osteoporosis: EndocrinologyDocument14 pagesLong-Term and Sequential Treatment For Osteoporosis: EndocrinologyjoaovcfNo ratings yet
- OsteoporosisDocument11 pagesOsteoporosis906 SoNo ratings yet
- Osteitis DeformansDocument4 pagesOsteitis Deformansmhuggnetoh19No ratings yet
- ORTHOPAEDICSDocument135 pagesORTHOPAEDICSJimmy MainaNo ratings yet
- Bisphosphonate Therapy: The Who, What, Why and HowDocument34 pagesBisphosphonate Therapy: The Who, What, Why and HowGayathri RaveendranNo ratings yet
- UK Guideline 2020 220709Document8 pagesUK Guideline 2020 220709rnwkrnrnNo ratings yet
- Osteoporosis: Mohd Fikri Bin MustapaDocument54 pagesOsteoporosis: Mohd Fikri Bin MustapaiqiessesNo ratings yet
- Articulo Bifosfonato en InglesDocument6 pagesArticulo Bifosfonato en InglesLeidy Marín SantanaNo ratings yet
- 111 Case Study 3Document3 pages111 Case Study 3jabyleynesNo ratings yet
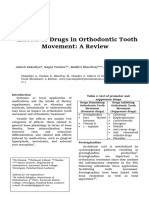
- Effects of Drugs in Orthodontic Tooth Movement: A ReviewDocument6 pagesEffects of Drugs in Orthodontic Tooth Movement: A ReviewvprakshaindiaNo ratings yet
- Four Types of Cells in BoneDocument5 pagesFour Types of Cells in BoneTazrian Islam FarihaNo ratings yet
- Osteo Notes 2Document2 pagesOsteo Notes 2api-273173999No ratings yet
- Osteoporosis: Causes, Symptoms and TreatmentDocument33 pagesOsteoporosis: Causes, Symptoms and TreatmentNadya LiemNo ratings yet
- Osteoporosis: Understanding the Silent Bone DiseaseDocument16 pagesOsteoporosis: Understanding the Silent Bone Diseasealaa azaweeNo ratings yet
- Osteoporosis: Causes, Incidence, and Risk FactorsDocument5 pagesOsteoporosis: Causes, Incidence, and Risk FactorsEmeka JusticeNo ratings yet
- What Is Osteopenia?: What Are Causes and Risk Factors For Osteopenia?Document2 pagesWhat Is Osteopenia?: What Are Causes and Risk Factors For Osteopenia?Jeremy EvansNo ratings yet
- OsteoporosisDocument9 pagesOsteoporosisRenuka Sivaram71% (7)
- Nursing Guide to Drugs Affecting the Endocrine SystemDocument58 pagesNursing Guide to Drugs Affecting the Endocrine SystemMuhammad Riandy Lukman TanjungNo ratings yet
- Drugs Used in OsteoporosisDocument30 pagesDrugs Used in Osteoporosissigit_riyantonoNo ratings yet
- Clinical Management of HypophosphatasiaDocument6 pagesClinical Management of HypophosphatasiaViknish ArumugamNo ratings yet
- Drugs in Orthodontics: G.Shekar Subramanian Ist Year PGDocument69 pagesDrugs in Orthodontics: G.Shekar Subramanian Ist Year PGShekar SubramanianNo ratings yet
- Urinary Tract InfectionDocument13 pagesUrinary Tract Infectiondiah poppy utamiNo ratings yet
- BISPHOSPHONATESDocument18 pagesBISPHOSPHONATEShumaNo ratings yet
- Bisphosphonates For OsteoporosisDocument4 pagesBisphosphonates For OsteoporosisNayem Hossain HemuNo ratings yet
- We Get Results!: BarreDocument36 pagesWe Get Results!: BarreCoolerAdsNo ratings yet
- 31 Day Dumbbell Bodyweight WorkoutDocument3 pages31 Day Dumbbell Bodyweight WorkoutSuvaneel MoulickNo ratings yet
- Date/Time Focus Progress Notes: Charisse Dl. LimosDocument6 pagesDate/Time Focus Progress Notes: Charisse Dl. LimosKish Dayanara GonzalesNo ratings yet
- 5 Ways For Improving Your Work-Life Balance: 1. Know That There Is No 'Perfect' BalanceDocument3 pages5 Ways For Improving Your Work-Life Balance: 1. Know That There Is No 'Perfect' BalanceDaniel Mathew VibyNo ratings yet
- Arm BP Differences Predict Early Death RiskDocument2 pagesArm BP Differences Predict Early Death RiskCarolina RusselNo ratings yet
- Classification and Causes of Anemia ExplainedDocument30 pagesClassification and Causes of Anemia ExplainedhercolaniumNo ratings yet
- Cleaner production assessment at Carm Foods EnterprisesDocument62 pagesCleaner production assessment at Carm Foods EnterprisesHarry EdnacotNo ratings yet
- BIOS LIFE - Diabetes in Control Study #2 by Steven Freed and David JoffeDocument1 pageBIOS LIFE - Diabetes in Control Study #2 by Steven Freed and David JoffeHisWellnessNo ratings yet
- Environment Institute of Malaysia (Eimas) Department of Environment MalaysiaDocument7 pagesEnvironment Institute of Malaysia (Eimas) Department of Environment MalaysiaCharlie EnvirochemNo ratings yet
- Rife Frequency List For Rife Frequency GeneratorDocument18 pagesRife Frequency List For Rife Frequency GeneratorAttila Dudás100% (2)
- Present Perfect PDFDocument2 pagesPresent Perfect PDFInma Polo TengoganasdefiestaNo ratings yet
- Indian Journal of Homoeopathic MedicineDocument29 pagesIndian Journal of Homoeopathic MedicineDinesh DhokeNo ratings yet
- ICU Assessment FormDocument6 pagesICU Assessment Formroro.8787.roroNo ratings yet
- Endoclear® Contributes To Decreasing Length of Stay in The ICUDocument1 pageEndoclear® Contributes To Decreasing Length of Stay in The ICUAlexandra HartNo ratings yet
- Medium ClinicDocument65 pagesMedium ClinicTeddy Million100% (1)
- OT Technician Syllabus GuideDocument11 pagesOT Technician Syllabus Guidehashir abbas100% (1)
- The Trauma of FreudDocument318 pagesThe Trauma of Freudrelsinger100% (5)
- Nursing Intervention and Smoking Cessation: A Meta-AnalysisDocument17 pagesNursing Intervention and Smoking Cessation: A Meta-AnalysisingevelystareslyNo ratings yet
- DOH-HFSRB-QOP01Form1 Rev2 6172022Document3 pagesDOH-HFSRB-QOP01Form1 Rev2 6172022clarisse salvadorNo ratings yet
- Types of Sutures and Their IndicationsDocument6 pagesTypes of Sutures and Their IndicationsAdina BurciuNo ratings yet
- Healing Spaces Elements of Environmental Design That Make An Impact On Health PDFDocument14 pagesHealing Spaces Elements of Environmental Design That Make An Impact On Health PDFCaesarC100% (1)
- James PRN This One THXDocument3 pagesJames PRN This One THXKaren MarcianoNo ratings yet
- Personality Styles and Brief PsychotherapyDocument135 pagesPersonality Styles and Brief PsychotherapyGeorgiana DetotNo ratings yet
- Case Presentation On Diabetic KetoacidosisDocument50 pagesCase Presentation On Diabetic KetoacidosisJoana Marie Gantuangco-MaglinteNo ratings yet
- A Comparative Clinical Study On The Effect of Kottamchukkadi and Kolakulathadi Upanaha Sweda in JanusandhigatavataDocument6 pagesA Comparative Clinical Study On The Effect of Kottamchukkadi and Kolakulathadi Upanaha Sweda in JanusandhigatavataInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- PsychoSocial Therapy TechniquesDocument9 pagesPsychoSocial Therapy TechniquesamitNo ratings yet
- Jurnal Internasional FlavonoidDocument8 pagesJurnal Internasional FlavonoidindahgamaNo ratings yet