You might also like
- Kırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisDocument40 pagesKırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisAli FalihNo ratings yet
- Ramel Pedro D. Tadong Post-Graduate Intern Department of PediatricsDocument5 pagesRamel Pedro D. Tadong Post-Graduate Intern Department of PediatricsJim Christian EllaserNo ratings yet
- Neonatal SepsisDocument5 pagesNeonatal SepsisBhawna PandhuNo ratings yet
- Neonatal Sepsis 1219225703095484 9Document50 pagesNeonatal Sepsis 1219225703095484 9Ali FalihNo ratings yet
- Fever With A Focus in Well Looking Child Under 3 YrsDocument80 pagesFever With A Focus in Well Looking Child Under 3 YrsAnuradha RoopchandNo ratings yet
- Neonatal InfectionsDocument41 pagesNeonatal Infectionsamid sultanNo ratings yet
- Sepsis Neonatal 2016Document102 pagesSepsis Neonatal 2016gcezcurraNo ratings yet
- Pediatric SepsisDocument57 pagesPediatric SepsisSondang Herikson PanjaitanNo ratings yet
- Neonatal Sepsis: - DR - Apoorva.E PG, DcmsDocument52 pagesNeonatal Sepsis: - DR - Apoorva.E PG, DcmsAli FalihNo ratings yet
- D1 - Theraputic Guidelines in Neonatal InfectionDocument15 pagesD1 - Theraputic Guidelines in Neonatal InfectiongaasheNo ratings yet
- Neonatal SepsisDocument38 pagesNeonatal SepsisJavier Saad100% (1)
- Ii. Epidemiological Description of Diseases: A. TuberculosisDocument13 pagesIi. Epidemiological Description of Diseases: A. TuberculosisChristine AlmoraNo ratings yet
- Approach To Child With Fever: Liew Qian YiDocument33 pagesApproach To Child With Fever: Liew Qian YinavenNo ratings yet
- Peadiatric Guildlines For Malaysian House OfficerDocument44 pagesPeadiatric Guildlines For Malaysian House OfficerAlex MatthewNo ratings yet
- Renal Transplant: 1) Steps Involved in Kidney TransplantationDocument4 pagesRenal Transplant: 1) Steps Involved in Kidney TransplantationNadia SalwaniNo ratings yet
- Kuliah Mahasiswan UPH, Neonatal SepsisDocument39 pagesKuliah Mahasiswan UPH, Neonatal Sepsiswilliam atmadjiNo ratings yet
- Communicable DiseasesDocument7 pagesCommunicable DiseasesRaisa Robelle Quicho100% (1)
- Neonatal SepsisDocument53 pagesNeonatal SepsisFrancis AmuzuNo ratings yet
- Module 14 Pediatric TB ENGLISHDocument85 pagesModule 14 Pediatric TB ENGLISHDellNo ratings yet
- Management of Neonatal SepsisDocument30 pagesManagement of Neonatal SepsisRam krishnaNo ratings yet
- Tuberculosis: Inhaled Droplet NucleiDocument4 pagesTuberculosis: Inhaled Droplet Nucleirhiesa75No ratings yet
- Neonatal SepsisDocument10 pagesNeonatal SepsisClaudelí GonzalezNo ratings yet
- Management of Neonatal Sepsis: Niki Kosmetatos, MD Anthony Piazza, MD J. Devn Cornish, MDDocument30 pagesManagement of Neonatal Sepsis: Niki Kosmetatos, MD Anthony Piazza, MD J. Devn Cornish, MDiniidzniNo ratings yet
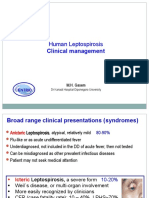
- Lepto Clinical Management GLEAN 2019 - M GasemDocument42 pagesLepto Clinical Management GLEAN 2019 - M GasemSelfie C RijalNo ratings yet
- Neonatal SepsisDocument51 pagesNeonatal SepsisAngelo Del VentoNo ratings yet
- History & Physical Exam in Ob/Gyn: By: - DR AmanuDocument75 pagesHistory & Physical Exam in Ob/Gyn: By: - DR AmanuKåbåñå TürüñåNo ratings yet
- Renal Transplant: 1) Steps Involved in Kidney TransplantationDocument4 pagesRenal Transplant: 1) Steps Involved in Kidney TransplantationNadia SalwaniNo ratings yet
- Recall ADocument86 pagesRecall ANikhil WaliaNo ratings yet
- UntitledDocument40 pagesUntitleddNo ratings yet
- Neonatal Sepsis: Prof DR Saima BatoolDocument31 pagesNeonatal Sepsis: Prof DR Saima BatoolSAIMA BATOOLNo ratings yet
- Neonatal SepsisDocument5 pagesNeonatal SepsisLeana SiñelNo ratings yet
- Clinical Practice Guideline On Neonatal Sepsis: Summarized by Dr. Catherine Chua October 2012Document3 pagesClinical Practice Guideline On Neonatal Sepsis: Summarized by Dr. Catherine Chua October 2012Joey CuayoNo ratings yet
- Gastroenteritis and ColitisDocument47 pagesGastroenteritis and ColitishaikalhjNo ratings yet
- San Lazaro Question Bank SouthPark 2Document9 pagesSan Lazaro Question Bank SouthPark 2Kenneth MiguelNo ratings yet
- Neonatal Sepsis: Author: Sherrill Roskam RNC MN NNP CNS Updated Presentation: Susan Greenleaf RNC, BSNDocument46 pagesNeonatal Sepsis: Author: Sherrill Roskam RNC MN NNP CNS Updated Presentation: Susan Greenleaf RNC, BSN'-dooublleaiienn Itouehh IinNo ratings yet
- 1.3 Demam Tifoid Dan Kelainan HeparDocument145 pages1.3 Demam Tifoid Dan Kelainan HeparajikwaNo ratings yet
- GRAND SGD For StudentsDocument3 pagesGRAND SGD For Studentsdonna dominnoNo ratings yet
- Part 1Document58 pagesPart 1Abdulrahman KatibNo ratings yet
- FeverDocument29 pagesFeverYogesh KharcheNo ratings yet
- Neonatal SepsisDocument31 pagesNeonatal Sepsisanwar jabariNo ratings yet
- Welcome To The Morning SessionDocument20 pagesWelcome To The Morning SessionGENERAL sharpNo ratings yet
- Omphalitis LectureDocument18 pagesOmphalitis LectureWonyenghitari George0% (1)
- Neonatal Infection: Julia PettyDocument15 pagesNeonatal Infection: Julia PettyVyshak KrishnanNo ratings yet
- Neonatal SepsisDocument20 pagesNeonatal SepsisNilanduniNo ratings yet
- Neonatal SepsisDocument24 pagesNeonatal SepsisEricson KipronoNo ratings yet
- 30131Document38 pages30131Virda MaharaniNo ratings yet
- Pediatric Hematology Oncology CaseDocument107 pagesPediatric Hematology Oncology CaseSayyed Ahmad KhursheedNo ratings yet
- 0002 Infectious Diseases of The HeartDocument35 pages0002 Infectious Diseases of The Heartmblanco.dchNo ratings yet
- Acute Lower Respiratory Tract Infection (ALRTI)Document43 pagesAcute Lower Respiratory Tract Infection (ALRTI)yosephNo ratings yet
- Asculitis Syndromes: Emily B. Martin, MD Rheumatology Board Review April 9, 2008Document54 pagesAsculitis Syndromes: Emily B. Martin, MD Rheumatology Board Review April 9, 2008Miguel M. Melchor RodríguezNo ratings yet
- Diseases, Syndromes & Health Events Under SurveillanceDocument61 pagesDiseases, Syndromes & Health Events Under SurveillanceGina BoligaoNo ratings yet
- Enteric FeverDocument7 pagesEnteric FeverkudzaimuregidubeNo ratings yet
- January 24 2006 TIME: 1hour Instructions To Candidates: Answer All Questions Answer Each Question in A Separate BookletDocument9 pagesJanuary 24 2006 TIME: 1hour Instructions To Candidates: Answer All Questions Answer Each Question in A Separate BookletAto Kwamena Sagoe100% (1)
- Clinical Presentation On Child With Neonatal SepsisDocument37 pagesClinical Presentation On Child With Neonatal SepsisSREEDEVI T SURESHNo ratings yet
- Enteric Fever 3Document33 pagesEnteric Fever 3Grethel H SobrepeñaNo ratings yet
- Topics For Oral Exam Thypoid FeverDrownTEFDocument2 pagesTopics For Oral Exam Thypoid FeverDrownTEFPCRMNo ratings yet
- A Case of Acute IdiopathicDocument19 pagesA Case of Acute IdiopathicSAIMA BATOOLNo ratings yet
- Puerperal SepsisDocument11 pagesPuerperal SepsisLana LocoNo ratings yet
- Guide to Pediatric Urology and Surgery in Clinical PracticeFrom EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNo ratings yet
- Blood and Tissue Flagellates para LecDocument8 pagesBlood and Tissue Flagellates para LecLian MallareNo ratings yet
- A Review On Health Benefit's of Pomegranate Flower.Document8 pagesA Review On Health Benefit's of Pomegranate Flower.StockerMarketNo ratings yet
- Faktor HospesDocument22 pagesFaktor Hospesari purwandiniNo ratings yet
- Image Production & Evaluation - HandoutDocument30 pagesImage Production & Evaluation - HandoutKarl Jay-Ronn GubocNo ratings yet
- Orthopedic Physical Assessment e Book Musculoskeletal Rehabilitation 6th Edition Ebook PDFDocument62 pagesOrthopedic Physical Assessment e Book Musculoskeletal Rehabilitation 6th Edition Ebook PDFkevin.smart540100% (43)
- Osteoporosis MergedDocument73 pagesOsteoporosis MergedrlpmanglicmotNo ratings yet
- DiabetesDocument31 pagesDiabetesIron ManNo ratings yet
- A Case Study ArticleDocument9 pagesA Case Study ArticleDr Prajakta BNo ratings yet
- Ward DrugsDocument5 pagesWard DrugsMary Grace AgataNo ratings yet
- Hematopoiesis: RbcsDocument27 pagesHematopoiesis: Rbcsjamba juiceNo ratings yet
- Chronic OsteomyelitisDocument49 pagesChronic OsteomyelitisBijay MehtaNo ratings yet
- Pulmonary Hypertension: Kazemi - Toba, M.D. Birjand University of Medical Sciences 24 Ordibeheshte 1390Document58 pagesPulmonary Hypertension: Kazemi - Toba, M.D. Birjand University of Medical Sciences 24 Ordibeheshte 1390Devashish VermaNo ratings yet
- Test Series For Neet-2020Document11 pagesTest Series For Neet-2020kavyareddyNo ratings yet
- Autoimmune - Hemolytic - Anemia - Mixed - Type-A - Case - Repo 2Document5 pagesAutoimmune - Hemolytic - Anemia - Mixed - Type-A - Case - Repo 2Afsha AnishNo ratings yet
- Amy Purdy - Listening ActivitiesDocument26 pagesAmy Purdy - Listening ActivitiesSelma NunesNo ratings yet
- Head To Toe Physical Examination PDFDocument24 pagesHead To Toe Physical Examination PDFCoasfan CossyNo ratings yet
- Kalsitonin PDFDocument12 pagesKalsitonin PDFFariz KasyidiNo ratings yet
- Educ5 Module4 Lesson5Document13 pagesEduc5 Module4 Lesson5Nj LangurayanNo ratings yet
- Sexually Transmitted DiseasesDocument9 pagesSexually Transmitted DiseasespromiseNo ratings yet
- Diagnostic Test For Endocrine DisordersDocument15 pagesDiagnostic Test For Endocrine DisordersRichard Deo R. Alave100% (1)
- Physical, Ergonomic and Psychosocial HazardsDocument64 pagesPhysical, Ergonomic and Psychosocial HazardsPatricia GalorioNo ratings yet
- CROSSWORD PUZZLE - Health ProblemsDocument4 pagesCROSSWORD PUZZLE - Health ProblemsVeZ xNo ratings yet
- 5 Aspirin CaseDocument40 pages5 Aspirin Caseمحمد القريضيNo ratings yet
- SchizophreniaDocument31 pagesSchizophreniaSheena PasionNo ratings yet
- F&E, Oxygenation - PreTestDocument9 pagesF&E, Oxygenation - PreTestToni Marie Buenconsejo PunzalanNo ratings yet
- Nursing Students Education During COVIDDocument2 pagesNursing Students Education During COVIDgotvelvet world dominationNo ratings yet
- Gallbladder Polyps - UpToDateDocument19 pagesGallbladder Polyps - UpToDateTrần Quốc KhánhNo ratings yet
- Neurological Assessment PDFDocument52 pagesNeurological Assessment PDFJosephine George JojoNo ratings yet
- BSBMED301: Assessment 1: What You Have To DoDocument8 pagesBSBMED301: Assessment 1: What You Have To DoPrayas AmatyaNo ratings yet
- CS Form 41 CSC Medical Certification PDFDocument1 pageCS Form 41 CSC Medical Certification PDFpearl cabugNo ratings yet