You might also like
- Normal Sinus RhythmDocument48 pagesNormal Sinus RhythmStella mNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Electrocardiograms (Ecgs)Document80 pagesElectrocardiograms (Ecgs)heena solankiNo ratings yet
- Simple Guide To Ecg InterpretationDocument53 pagesSimple Guide To Ecg Interpretationedy suyantoNo ratings yet
- Basics of ECG: By-Pallavi ChicholikarDocument115 pagesBasics of ECG: By-Pallavi ChicholikarBhakti WashilkarNo ratings yet
- Basics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyDocument206 pagesBasics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyRavi SharmaNo ratings yet
- Kuliah EKG Blok Kegawatdaruratan September 2018Document122 pagesKuliah EKG Blok Kegawatdaruratan September 2018khanzaisdiharanaNo ratings yet
- Electrocardiogram (E.C.G)Document51 pagesElectrocardiogram (E.C.G)Jamuna PatelNo ratings yet
- EKG Interpretasi Dan Lethal Aritmia: Aan NuraeniDocument34 pagesEKG Interpretasi Dan Lethal Aritmia: Aan NuraeniCitra Marchelina Novilini100% (1)
- ELECTROCARDIOGRAMDocument63 pagesELECTROCARDIOGRAMMbah GapinbissiNo ratings yet
- Acute Coronary SyndromeDocument79 pagesAcute Coronary SyndromeMuhammad Yufimar Rizza FadilahNo ratings yet
- Ecg BSTDocument204 pagesEcg BSTAnusha Verghese100% (1)
- Asist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasDocument64 pagesAsist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasAnonymous CQmrhq1O7No ratings yet
- ELECTROCARDIOGRAPHYDocument75 pagesELECTROCARDIOGRAPHYMeliaNo ratings yet
- Electrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHDocument42 pagesElectrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHNorPhea - នភាNo ratings yet
- PDF DocumentDocument40 pagesPDF DocumentsalikiqbalNo ratings yet
- Presentasi Ws Ekg SakinahDocument40 pagesPresentasi Ws Ekg SakinahsiskaNo ratings yet
- THE Electrocardiogram (Ecg / Ekg) : By: DR Yasir MansouriDocument83 pagesTHE Electrocardiogram (Ecg / Ekg) : By: DR Yasir Mansourirofi modiNo ratings yet
- ECGDocument198 pagesECGKatrina Maravilla100% (1)
- Ecg Interpretation:: The BasicsDocument40 pagesEcg Interpretation:: The BasicsRavi SharmaNo ratings yet
- How To Read An EcgDocument86 pagesHow To Read An EcgmajdNo ratings yet
- BCS EkgDocument55 pagesBCS Ekggita suariyaniNo ratings yet
- Normal ECGDocument63 pagesNormal ECGMohd Johari Mohd ShafuwanNo ratings yet
- EkgDocument67 pagesEkgFendi Rafif Dad'sNo ratings yet
- ECG ArrythemiaDocument79 pagesECG ArrythemiaMahadevNo ratings yet
- ELEKTROKARDIOGRAFI Ridwan 2018Document90 pagesELEKTROKARDIOGRAFI Ridwan 2018YogaNo ratings yet
- The Normal ElectrocardiogramDocument63 pagesThe Normal ElectrocardiogramPuravin Crishan VeerasamyNo ratings yet
- Basic of ECG: Prepared By: Zahid HussainDocument38 pagesBasic of ECG: Prepared By: Zahid HussainZahid Hussain100% (1)
- APEC 611 Scientific and Industrial Instrumentation: Electrocardiogram (ECG)Document22 pagesAPEC 611 Scientific and Industrial Instrumentation: Electrocardiogram (ECG)Faisal Bin KashemNo ratings yet
- Jose Gianni C. Espada Clinical ClerkDocument133 pagesJose Gianni C. Espada Clinical ClerkJohn Christopher LucesNo ratings yet
- Basic Concepts of Clinical ECGDocument40 pagesBasic Concepts of Clinical ECGArslan KhanNo ratings yet
- Lectro Ardio Raphy: by Dr. Omprakash Sah Medical Officer NAMS, Bir HospitalDocument162 pagesLectro Ardio Raphy: by Dr. Omprakash Sah Medical Officer NAMS, Bir HospitalAjay SharmaNo ratings yet
- ElectrocardiogramDocument169 pagesElectrocardiogramjitendra magarNo ratings yet
- Interpretasi ElektrokardiogramDocument36 pagesInterpretasi ElektrokardiogramendahNo ratings yet
- ECG InterpretationDocument73 pagesECG Interpretationsultan khabeebNo ratings yet
- ECGDocument41 pagesECGmiguel mendezNo ratings yet
- Didactics ECGDocument87 pagesDidactics ECGGenesis Poblacion100% (1)
- ECG InterpretationDocument95 pagesECG InterpretationNur Rahmat Wibowo100% (9)
- Ecg Interpretation: Gowtham Krishna JDocument60 pagesEcg Interpretation: Gowtham Krishna JGowtham KrishnaNo ratings yet
- EcgDocument6 pagesEcgMohamed IbrahimNo ratings yet
- Cardio INTERPRETATION OF THE ELECTROCARDIOGRAMDocument74 pagesCardio INTERPRETATION OF THE ELECTROCARDIOGRAMkrisnoNo ratings yet
- Electrocardiography: DR Uwanuruochi KelechukwuDocument50 pagesElectrocardiography: DR Uwanuruochi KelechukwuJake MillerNo ratings yet
- Basic ECG ReadingDocument41 pagesBasic ECG ReadingBenj100% (4)
- DrAbnet ECG - BasicsDocument99 pagesDrAbnet ECG - BasicsAbnet WondimuNo ratings yet
- Interpretasi ElektrokardiografiDocument60 pagesInterpretasi ElektrokardiografiYogi GustriansyahNo ratings yet
- Cme Ecg InterpretationDocument60 pagesCme Ecg InterpretationAtirah AaNo ratings yet
- Cardiocon ECG Workshop Basics of ECGDocument80 pagesCardiocon ECG Workshop Basics of ECGshazia kaziNo ratings yet
- Tomasz WikarekDocument95 pagesTomasz Wikareknamar13766No ratings yet
- Electrocardiograms (Ecgs)Document86 pagesElectrocardiograms (Ecgs)nana wandhanaNo ratings yet
- Basic ECG For ParamedicDocument82 pagesBasic ECG For ParamedicMaza AmfoterikNo ratings yet
- ECG - Doc 09Document11 pagesECG - Doc 09Rincy RajanNo ratings yet
- Elektro Kardio Grafi - Dasar - : DR Eka Ginanjar, SPPDDocument105 pagesElektro Kardio Grafi - Dasar - : DR Eka Ginanjar, SPPDalmiraerickaiNo ratings yet
- Kuliah Ekg UnswagatiDocument75 pagesKuliah Ekg UnswagatiiikNo ratings yet
- Basic ECG Lecture - NewDocument148 pagesBasic ECG Lecture - NewAradhanaRamchandaniNo ratings yet
- INTERPRETASI EKG MahasiswaDocument43 pagesINTERPRETASI EKG MahasiswaMartin Susanto, MDNo ratings yet
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocument74 pagesBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- ECG Normal - ErwanDocument49 pagesECG Normal - ErwanEvelyne NatalieNo ratings yet
- Pemasangan Dan Interpretasi EKGDocument117 pagesPemasangan Dan Interpretasi EKGaulianadanisya100% (2)
- Ecg Interpretation New TemplateDocument88 pagesEcg Interpretation New TemplateJonathan NgNo ratings yet
- Transient Ischemic Attack Precipitating Factors Predisposing FactorsDocument6 pagesTransient Ischemic Attack Precipitating Factors Predisposing FactorsYosef OxinioNo ratings yet
- Christopher Cheung Approach To Cardiac History Taking: Cyanosis or SyncopeDocument6 pagesChristopher Cheung Approach To Cardiac History Taking: Cyanosis or SyncopeApryl Phyllis JimenezNo ratings yet
- The ECG Made Easy by John R. HamptonDocument1 pageThe ECG Made Easy by John R. HamptonLpNo ratings yet
- Debra Laurent HandoutDocument23 pagesDebra Laurent Handoutrrs111rrsNo ratings yet
- Atrial RhythmDocument12 pagesAtrial RhythmMashhoora jahanNo ratings yet
- SCDDocument41 pagesSCDhendra2darmawan100% (1)
- Cryptogenic StrokeDocument52 pagesCryptogenic Strokemrabhilekh100% (1)
- CVD in Diabetes - EADSG 2016Document57 pagesCVD in Diabetes - EADSG 2016OmarNo ratings yet
- Pericardial DX Endocarditis MyocarditisDocument63 pagesPericardial DX Endocarditis MyocarditisIrfan Ners MaulanaNo ratings yet
- Cardiology Basic QuestionsDocument9 pagesCardiology Basic QuestionsSunita PooniaNo ratings yet
- Myocardial InfarctionDocument1 pageMyocardial InfarctionjljoioiuNo ratings yet
- Coarctation of The AortaDocument26 pagesCoarctation of The AortaMissDyYournurseNo ratings yet
- Neurologic Disorders Associated With Mitral Valve ProlapseDocument6 pagesNeurologic Disorders Associated With Mitral Valve Prolapsegeorgiana_884431330No ratings yet
- PKB 2021 Compiled NewDocument264 pagesPKB 2021 Compiled Newfrengki prasNo ratings yet
- Case Presentation - Aortic StenosisDocument31 pagesCase Presentation - Aortic Stenosissharathpaps0% (1)
- Hypertensive Heart DiseaseDocument18 pagesHypertensive Heart DiseaseKaye ViolaNo ratings yet
- Cardiology. Scheme ..Dof3tna - Net... EgyDrDocument4 pagesCardiology. Scheme ..Dof3tna - Net... EgyDrJilan El SherBiny100% (1)
- CVS-01 Examination & Short CasesDocument9 pagesCVS-01 Examination & Short Casesem khanNo ratings yet
- 20 Anesthesia For Congenital Heart SurgeryDocument69 pages20 Anesthesia For Congenital Heart Surgerypioja22507No ratings yet
- Stroke PathophysiologyDocument1 pageStroke PathophysiologyBram AderNo ratings yet
- Mitral Valve Disease: A Comprehensive ReviewDocument8 pagesMitral Valve Disease: A Comprehensive ReviewArthurNo ratings yet
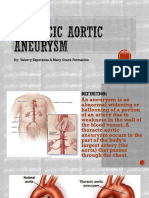
- Thoracic Aortic AneurysmDocument17 pagesThoracic Aortic AneurysmGlyssa CabarrubiasNo ratings yet
- Cardio Vascular & Thoracic Surgery (Direct 6 Years Course) Part - I Paper-IiDocument2 pagesCardio Vascular & Thoracic Surgery (Direct 6 Years Course) Part - I Paper-Iilakshminivas PingaliNo ratings yet
- Clinical Exam NotesDocument222 pagesClinical Exam Notesakansha_bhargava_6100% (1)
- Cardiac Physical ExamDocument45 pagesCardiac Physical ExamARIANNE JOY TAMARAY100% (1)
- Athlete's Heart: Dr. Arzalan BaigDocument59 pagesAthlete's Heart: Dr. Arzalan BaigArzalan BaigNo ratings yet
- Pakya ECG BasicsDocument5 pagesPakya ECG BasicsFrederick CokroNo ratings yet
- Ischemic Stroke: Let's Talk AboutDocument2 pagesIschemic Stroke: Let's Talk AboutMarhaban WienNo ratings yet
- NCP Ineffective Cardiopulmonary PerfusionDocument3 pagesNCP Ineffective Cardiopulmonary PerfusionjamiemapanaoNo ratings yet
- Vasovagal SyncopeDocument13 pagesVasovagal SyncopeEmily EresumaNo ratings yet