You might also like
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- ELECTROCARDIOGRAPHYDocument75 pagesELECTROCARDIOGRAPHYMeliaNo ratings yet
- ECG Basics and Normal ECG PatternsDocument40 pagesECG Basics and Normal ECG PatternsArslan KhanNo ratings yet
- Ecg Interpretation:: The BasicsDocument40 pagesEcg Interpretation:: The BasicsRavi SharmaNo ratings yet
- Normal Sinus RhythmDocument48 pagesNormal Sinus RhythmStella mNo ratings yet
- PDF DocumentDocument40 pagesPDF DocumentsalikiqbalNo ratings yet
- DrAbnet ECG - BasicsDocument99 pagesDrAbnet ECG - BasicsAbnet WondimuNo ratings yet
- ECG ECG Basics Presentation 201309101527422446 PDFDocument45 pagesECG ECG Basics Presentation 201309101527422446 PDFRamesh RajNo ratings yet
- A Simple Guide to ECG InterpretationDocument53 pagesA Simple Guide to ECG Interpretationedy suyantoNo ratings yet
- ECG InterpretationDocument73 pagesECG Interpretationsultan khabeebNo ratings yet
- Elektrokardiografi Dasar: Dr. Eka Ginanjar, SPPDDocument81 pagesElektrokardiografi Dasar: Dr. Eka Ginanjar, SPPDNur Rahmat WibowoNo ratings yet
- ECG ArrythemiaDocument79 pagesECG ArrythemiaMahadevNo ratings yet
- Kuliah EKG Blok Kegawatdaruratan September 2018Document122 pagesKuliah EKG Blok Kegawatdaruratan September 2018khanzaisdiharanaNo ratings yet
- Basics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyDocument206 pagesBasics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyRavi SharmaNo ratings yet
- Electrical Activity of The HeartDocument156 pagesElectrical Activity of The HeartNIRANJANA SHALININo ratings yet
- ECGDocument115 pagesECGBhakti WashilkarNo ratings yet
- Normal Ecg ReportDocument27 pagesNormal Ecg ReportMark DycNo ratings yet
- Asist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasDocument64 pagesAsist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasAnonymous CQmrhq1O7No ratings yet
- Dr. Anas Yasin - MDDocument58 pagesDr. Anas Yasin - MDMahfouzNo ratings yet
- How To Read An EcgDocument86 pagesHow To Read An EcgmajdNo ratings yet
- Electrical Impulse Viewed: Interpretation of The ElectrocardiogramDocument41 pagesElectrical Impulse Viewed: Interpretation of The ElectrocardiogramNesru Ahmed AkkichuNo ratings yet
- ECG - Doc 09Document11 pagesECG - Doc 09Rincy RajanNo ratings yet
- Lectro Ardio Raphy: by Dr. Omprakash Sah Medical Officer NAMS, Bir HospitalDocument162 pagesLectro Ardio Raphy: by Dr. Omprakash Sah Medical Officer NAMS, Bir HospitalAjay SharmaNo ratings yet
- THE NORMAL ELECTROCARDIOGRAM: DIAGNOSING MEDICAL PROBLEMS WITH AN ECGDocument63 pagesTHE NORMAL ELECTROCARDIOGRAM: DIAGNOSING MEDICAL PROBLEMS WITH AN ECGPuravin Crishan VeerasamyNo ratings yet
- ECG Interpretation GuideDocument50 pagesECG Interpretation GuideJake MillerNo ratings yet
- Ecg Interpretation: Gowtham Krishna JDocument60 pagesEcg Interpretation: Gowtham Krishna JGowtham KrishnaNo ratings yet
- Ecg Basics - NAVEENDocument65 pagesEcg Basics - NAVEENNaveen MathieuNo ratings yet
- EcgDocument6 pagesEcgMohamed IbrahimNo ratings yet
- Ecg BSTDocument204 pagesEcg BSTAnusha Verghese100% (1)
- Kuliah Ekg UnswagatiDocument75 pagesKuliah Ekg UnswagatiiikNo ratings yet
- ECG Basics: An Overview of ElectrocardiographyDocument51 pagesECG Basics: An Overview of ElectrocardiographyJamuna PatelNo ratings yet
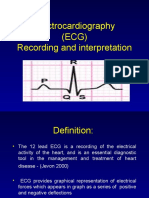
- Electrocardiography (ECG) Recording and InterpretationDocument59 pagesElectrocardiography (ECG) Recording and Interpretationkhushsandhu0% (1)
- ECG ECG Basics PresentationDocument45 pagesECG ECG Basics PresentationLan Anh Pham100% (1)
- Electrocardiography: Is Recording and Study of Electrical CurrentDocument107 pagesElectrocardiography: Is Recording and Study of Electrical CurrentkedirNo ratings yet
- ECGDocument41 pagesECGmiguel mendezNo ratings yet
- Ecg Interpretation New TemplateDocument88 pagesEcg Interpretation New TemplateJonathan NgNo ratings yet
- Electrophysiology of The HeartDocument27 pagesElectrophysiology of The HeartTsegaye HailuNo ratings yet
- EKG 12 Lead GuideDocument59 pagesEKG 12 Lead GuideM Lukman HakimNo ratings yet
- ECGDocument198 pagesECGKatrina Maravilla100% (1)
- Understanding Basics of EKG: by Alula A. (R III)Document37 pagesUnderstanding Basics of EKG: by Alula A. (R III)sky nutsNo ratings yet
- ECG InterpretationDocument95 pagesECG InterpretationNur Rahmat Wibowo100% (9)
- Lab Exercise 5 PDFDocument50 pagesLab Exercise 5 PDFE1- Villapaz, Aiemarie R. (Aie)No ratings yet
- ECG FILEDocument29 pagesECG FILEneha miriNo ratings yet
- ECGDocument33 pagesECGWasif RaheelNo ratings yet
- Cardiocon ECG Workshop Basics of ECGDocument80 pagesCardiocon ECG Workshop Basics of ECGshazia kaziNo ratings yet
- ECG InterpretationDocument40 pagesECG InterpretationMuhammad BadrushshalihNo ratings yet
- Unit-2 ECG LNRDocument29 pagesUnit-2 ECG LNRNagarajan LNo ratings yet
- Basic ECG LectureDocument148 pagesBasic ECG LectureAradhanaRamchandaniNo ratings yet
- ECG Guide: Anatomy, Physiology, Interpretation and AbnormalitiesDocument102 pagesECG Guide: Anatomy, Physiology, Interpretation and AbnormalitiesMustafa A. DawoodNo ratings yet
- Cardio INTERPRETATION OF THE ELECTROCARDIOGRAMDocument74 pagesCardio INTERPRETATION OF THE ELECTROCARDIOGRAMkrisnoNo ratings yet
- KULIAH ECG Dinkes PurworejoDocument69 pagesKULIAH ECG Dinkes PurworejoVella NurfatimahNo ratings yet
- KULIAH ECG Dinkes PurworejoDocument69 pagesKULIAH ECG Dinkes PurworejoSofian PalupiNo ratings yet
- APEC 611 Scientific and Industrial Instrumentation: Electrocardiogram (ECG)Document22 pagesAPEC 611 Scientific and Industrial Instrumentation: Electrocardiogram (ECG)Faisal Bin KashemNo ratings yet
- EcgDocument18 pagesEcgmyla adapNo ratings yet
- How To Take and Read An ECG ECG BasicsDocument7 pagesHow To Take and Read An ECG ECG BasicsJessica Brittain-GeorgeNo ratings yet
- Cardiac Arrest: April B. Perez, RN, Man, PHD, FpchaDocument50 pagesCardiac Arrest: April B. Perez, RN, Man, PHD, Fpchayuuki konnoNo ratings yet
- ECGDocument70 pagesECGgemergencycareNo ratings yet
- Electrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHDocument42 pagesElectrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHNorPhea - នភាNo ratings yet
- DASAR KURSUS EKG - DR WiryawanDocument68 pagesDASAR KURSUS EKG - DR WiryawanElsa TjahyaNo ratings yet
- Alabama GroupDocument3 pagesAlabama GroupYogaNo ratings yet
- Aktivitas Fisik Pada Dewasa Dan GeriatriDocument21 pagesAktivitas Fisik Pada Dewasa Dan GeriatriYogaNo ratings yet
- Tugas Akhir Bahasa Inggris Opini KesehatanDocument1 pageTugas Akhir Bahasa Inggris Opini KesehatanYogaNo ratings yet
- Tugas Akhir Bahasa Inggris Opini KesehatanDocument1 pageTugas Akhir Bahasa Inggris Opini KesehatanYogaNo ratings yet
- Tugas Bahasa Inggris Cerita RakyatDocument1 pageTugas Bahasa Inggris Cerita RakyatYogaNo ratings yet
- Wa0017 PDFDocument1 pageWa0017 PDFYogaNo ratings yet
- Tugas Bahasa Inggris Cerita RakyatDocument1 pageTugas Bahasa Inggris Cerita RakyatYogaNo ratings yet
- Tugas Mku Bahasa Inggris Nama:: Yoga Ichlassul AmalDocument5 pagesTugas Mku Bahasa Inggris Nama:: Yoga Ichlassul AmalYogaNo ratings yet
- Kuliah Pakar Komunikasi Interpersonal, Etika Dan Profesionalisme DokterDocument46 pagesKuliah Pakar Komunikasi Interpersonal, Etika Dan Profesionalisme DokterYogaNo ratings yet
- 2012 EO2 Student HB v1.0Document78 pages2012 EO2 Student HB v1.0Ariane HoffmannNo ratings yet
- Pericardial EffusionDocument41 pagesPericardial Effusionanon_516278156No ratings yet
- Medical Assistant Study Guide PDFDocument116 pagesMedical Assistant Study Guide PDFFelishaBassettNo ratings yet
- Development of An Advanced Gene Therapy For The Treatment of Hereditary Heart Diseases in CaninesDocument17 pagesDevelopment of An Advanced Gene Therapy For The Treatment of Hereditary Heart Diseases in CaninesAnawhatNo ratings yet
- Rundown WORKSHOP BKCU 2023-REVISI UPDATEDocument8 pagesRundown WORKSHOP BKCU 2023-REVISI UPDATEacengNo ratings yet
- Serbia ACS Incidence and Mortality 2010Document127 pagesSerbia ACS Incidence and Mortality 2010Poledica MladenNo ratings yet
- DIABETES Nursing ManagementDocument11 pagesDIABETES Nursing ManagementKaloy KamaoNo ratings yet
- Case Study (Muscular)Document11 pagesCase Study (Muscular)Yusra Angel DelfinNo ratings yet
- 10clinical VignettespdfDocument71 pages10clinical VignettespdfKerin Ardy100% (1)
- 6 Pack Sept 2013-OEC-Shock-Chapter 10 - NSPDocument23 pages6 Pack Sept 2013-OEC-Shock-Chapter 10 - NSPDonavon GaudetteNo ratings yet
- HOSPITAL DEPTS GUIDEDocument16 pagesHOSPITAL DEPTS GUIDEfictoriaNo ratings yet
- Iloilo Doctors' College College of Nursing: West Avenue, Molo, Iloilo CityDocument2 pagesIloilo Doctors' College College of Nursing: West Avenue, Molo, Iloilo CityAudrie Allyson GabalesNo ratings yet
- ANP Heart Anatomy & PhysiologyDocument3 pagesANP Heart Anatomy & PhysiologySheana Tmpl100% (1)
- Diagnostic Challenges and Uncertainties of Embolic Strokes of UndeterminedDocument4 pagesDiagnostic Challenges and Uncertainties of Embolic Strokes of UndeterminedDarliana Ospina DuarteNo ratings yet
- Medical Nutrition Therapy A Case Study Approach 5th Edition Nelms Solutions ManualDocument8 pagesMedical Nutrition Therapy A Case Study Approach 5th Edition Nelms Solutions Manualsophiechaurfqnz100% (31)
- CCLS IRC ISA CPR Guidelines PPT Rakesh GargDocument67 pagesCCLS IRC ISA CPR Guidelines PPT Rakesh GargPiyush JoshiNo ratings yet
- 304 FullDocument9 pages304 FullIcicNo ratings yet
- Autopsy PDFDocument3 pagesAutopsy PDFstprepsNo ratings yet
- Clinical CoachDocument374 pagesClinical CoachGensai KawakamiNo ratings yet
- Hendra - EKGDocument34 pagesHendra - EKGRINANo ratings yet
- Materi 3 - WS Exercise Stress TestDocument22 pagesMateri 3 - WS Exercise Stress TestMaria ulfahNo ratings yet
- ICU Lines TubesDocument7 pagesICU Lines TubesCindy MurphyNo ratings yet
- Final - Exam - 6512N - EXAM 1Document13 pagesFinal - Exam - 6512N - EXAM 1erick kanyi100% (1)
- Pre-Board Papers With MS ScienceDocument323 pagesPre-Board Papers With MS Scienceayishasamath08No ratings yet
- Aortic Valve Disease, Transcatheter Aortic Valve Replacement, and The Heart Failure Patient A State-Of-The-Art ReviewDocument14 pagesAortic Valve Disease, Transcatheter Aortic Valve Replacement, and The Heart Failure Patient A State-Of-The-Art ReviewCarlos Alberto Holguin PalaciosNo ratings yet
- Clinical Standards For Heart Disease 2010Document59 pagesClinical Standards For Heart Disease 2010Novita Dwi MardiningtyasNo ratings yet
- Boericke Tinctures PDFDocument136 pagesBoericke Tinctures PDFitsokok100% (2)
- Based On The Case, Assess The Patient's Asthma Control According To The Two Domains: 1. Symptom Control 2. Future Risk of Adverse OutcomesDocument7 pagesBased On The Case, Assess The Patient's Asthma Control According To The Two Domains: 1. Symptom Control 2. Future Risk of Adverse OutcomesNicole BaysaNo ratings yet
- Curriculum BS MLT IIMCDocument106 pagesCurriculum BS MLT IIMCAmna Zafar100% (1)
- @anesthesia Books 2017 EssentialsDocument346 pages@anesthesia Books 2017 EssentialsAnonymous EQnqbCTNo ratings yet