You might also like
- ECG Basics Module-1Document127 pagesECG Basics Module-1manyusinghNo ratings yet
- Temperature Pulse + RespirationsDocument2 pagesTemperature Pulse + RespirationsMarshin Thea Celocia100% (1)
- Simple Guide To Ecg InterpretationDocument53 pagesSimple Guide To Ecg Interpretationedy suyantoNo ratings yet
- ECGDocument41 pagesECGmiguel mendezNo ratings yet
- About The Heart and Blood Vessels Anatomy and Function of The Heart ValvesDocument4 pagesAbout The Heart and Blood Vessels Anatomy and Function of The Heart ValvesdomlhynNo ratings yet
- Cardiovascular Physiology - Cardiac Cycle and MurmursDocument107 pagesCardiovascular Physiology - Cardiac Cycle and MurmursAaron D. Phoenix100% (1)
- Santosh DevDocument45 pagesSantosh Devdevdsantosh100% (1)
- Ecg Treadmill and Holter TestDocument77 pagesEcg Treadmill and Holter TestRiteka Singh100% (1)
- BLS Provider ManualDocument23 pagesBLS Provider ManualMaya LaPrade100% (3)
- ECG InterpretationDocument73 pagesECG Interpretationsultan khabeebNo ratings yet
- Basic EKG InterpretationDocument48 pagesBasic EKG InterpretationAimee Ann Pauco MacaraegNo ratings yet
- Basic Ecg Interpretation and Arrhythmia Recognition By: Ma. Victoria E. Martinez Er - RNDocument34 pagesBasic Ecg Interpretation and Arrhythmia Recognition By: Ma. Victoria E. Martinez Er - RNMavic Martinez BuntalesNo ratings yet
- CPM15th HYPERTENSION (PSH) PDFDocument14 pagesCPM15th HYPERTENSION (PSH) PDFlouie john abilaNo ratings yet
- Vagus Nerve StimulationDocument2 pagesVagus Nerve StimulationMary Antonette100% (2)
- Ecg Interpretation: Presented by:-ROHINI RAI M SC Nursing Part I, C.O.N, N.B.M.C.HDocument69 pagesEcg Interpretation: Presented by:-ROHINI RAI M SC Nursing Part I, C.O.N, N.B.M.C.HRohini RaiNo ratings yet
- Lecture On Basics of ECG For 1st Year MBBS by Dr. RoomiDocument28 pagesLecture On Basics of ECG For 1st Year MBBS by Dr. RoomiMudassar Roomi100% (3)
- Basic ECG Lecture - NewDocument148 pagesBasic ECG Lecture - NewAradhanaRamchandaniNo ratings yet
- Asist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasDocument64 pagesAsist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasAnonymous CQmrhq1O7No ratings yet
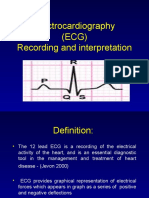
- Electrocardiography (ECG) Recording and InterpretationDocument59 pagesElectrocardiography (ECG) Recording and Interpretationkhushsandhu0% (1)
- Cardiac Output and Hemodynamic MeasurementDocument29 pagesCardiac Output and Hemodynamic Measurementdeepa100% (1)
- Basics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyDocument206 pagesBasics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyRavi SharmaNo ratings yet
- HandBook of Pathology and PathoPhysiology of CardioVascularDocument321 pagesHandBook of Pathology and PathoPhysiology of CardioVascularNurwahidah Moh WahiNo ratings yet
- Unit-2 ECG LNRDocument29 pagesUnit-2 ECG LNRNagarajan LNo ratings yet
- ECG1Document67 pagesECG1Farhan RosliNo ratings yet
- Adrenergic AgonistsDocument52 pagesAdrenergic AgonistsTsegaye HailuNo ratings yet
- Lectro Ardio Raphy: by Dr. Omprakash Sah Medical Officer NAMS, Bir HospitalDocument162 pagesLectro Ardio Raphy: by Dr. Omprakash Sah Medical Officer NAMS, Bir HospitalAjay SharmaNo ratings yet
- Hyperbaric Oxygen Therapy For Acute Coronary SyndromeDocument29 pagesHyperbaric Oxygen Therapy For Acute Coronary Syndromedevi agustinNo ratings yet
- Electrocardiography: DR Uwanuruochi KelechukwuDocument50 pagesElectrocardiography: DR Uwanuruochi KelechukwuJake MillerNo ratings yet
- MUCLecture 2021 1292271Document34 pagesMUCLecture 2021 1292271Kouka MahfoudiNo ratings yet
- Ecg PrsentationDocument33 pagesEcg Prsentationtehillahkabwe100No ratings yet
- Normal Sinus RhythmDocument48 pagesNormal Sinus RhythmStella mNo ratings yet
- ECG Complete LectureDocument33 pagesECG Complete LectureDr. SUVA NATHNo ratings yet
- Mechanical and Electrical Events of The Cardiac CycleDocument39 pagesMechanical and Electrical Events of The Cardiac CyclebhatsindhoorNo ratings yet
- Electrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHDocument42 pagesElectrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHNorPhea - នភាNo ratings yet
- Lab Exercise 5 PDFDocument50 pagesLab Exercise 5 PDFE1- Villapaz, Aiemarie R. (Aie)No ratings yet
- Electrical Activity of The HeartDocument156 pagesElectrical Activity of The HeartNIRANJANA SHALININo ratings yet
- Basic Concepts of Clinical ECGDocument40 pagesBasic Concepts of Clinical ECGArslan KhanNo ratings yet
- Electrocardiogram (2022) )Document128 pagesElectrocardiogram (2022) )Craft Hachz By dhiyaNo ratings yet
- ELEKTROKARDIOGRAFI Ridwan 2018Document90 pagesELEKTROKARDIOGRAFI Ridwan 2018YogaNo ratings yet
- How To Read An EcgDocument86 pagesHow To Read An EcgmajdNo ratings yet
- The Electrocardiogram: Ecg: by Gaurishi Agarwal, 32Document17 pagesThe Electrocardiogram: Ecg: by Gaurishi Agarwal, 32Gaurishi AgarwalNo ratings yet
- Ecg BSTDocument204 pagesEcg BSTAnusha Verghese100% (1)
- ECG EKG: BasicsDocument191 pagesECG EKG: BasicsSabio DenmenNo ratings yet
- Electrical Impulse Viewed: Interpretation of The ElectrocardiogramDocument41 pagesElectrical Impulse Viewed: Interpretation of The ElectrocardiogramNesru Ahmed AkkichuNo ratings yet
- Electrocardiogram (ECG) : This Is The Lecture No. 4Document51 pagesElectrocardiogram (ECG) : This Is The Lecture No. 4Aboodsha ShNo ratings yet
- Matrikulasi Interpretasi EkgDocument40 pagesMatrikulasi Interpretasi Ekgsupergirl2123No ratings yet
- Electrocardiogram: By: Keverne Jhay P. Colas, RN, MANDocument72 pagesElectrocardiogram: By: Keverne Jhay P. Colas, RN, MANGaras AnnaBerniceNo ratings yet
- EcgDocument18 pagesEcgmyla adapNo ratings yet
- Ecg Physio LectureDocument60 pagesEcg Physio LectureAninze Chidera100% (1)
- Electrical Activity of The HeartDocument40 pagesElectrical Activity of The HeartMichael Ajak GhaiNo ratings yet
- CVS 1 Cardiac CycleDocument29 pagesCVS 1 Cardiac CycleDedani MakakaNo ratings yet
- DrAbnet ECG - BasicsDocument99 pagesDrAbnet ECG - BasicsAbnet WondimuNo ratings yet
- DYSRHYTMIASDocument16 pagesDYSRHYTMIASVictor StevenNo ratings yet
- Electrocardiography Basic: DR Budi EnochDocument49 pagesElectrocardiography Basic: DR Budi EnochYohanes Malindo Wiyaa DBs-uno100% (1)
- Ecg Basics - NAVEENDocument65 pagesEcg Basics - NAVEENNaveen MathieuNo ratings yet
- Ecg or Electro Cardiogram and ElectrocardiographDocument20 pagesEcg or Electro Cardiogram and ElectrocardiographsureshNo ratings yet
- ECG - Doc 09Document11 pagesECG - Doc 09Rincy RajanNo ratings yet
- Mechanical and Electrical Events of The Cardiac CycleDocument39 pagesMechanical and Electrical Events of The Cardiac CycleEdi HidayatNo ratings yet
- Electrocardiography: An Introduction To The ECGDocument76 pagesElectrocardiography: An Introduction To The ECGInnocent Clifford MaranduNo ratings yet
- Ecg 1Document198 pagesEcg 1hibaNo ratings yet
- ECG PracticalDocument48 pagesECG PracticalbvkjtzrvnyNo ratings yet
- Normal Ecg ReportDocument27 pagesNormal Ecg ReportMark DycNo ratings yet
- Electrocardiography: DR Budi EnochDocument115 pagesElectrocardiography: DR Budi EnochAriyanaNo ratings yet
- Department of Cardiology and Vascular Medicine, Padjadjaran University School of Medicine Hasan Sadikin Hospital BandungDocument61 pagesDepartment of Cardiology and Vascular Medicine, Padjadjaran University School of Medicine Hasan Sadikin Hospital BandungMuhammad AmrieNo ratings yet
- Lec7 Sem2 CVSWK3 20140920 PDFDocument12 pagesLec7 Sem2 CVSWK3 20140920 PDFAprina RosyadahNo ratings yet
- EcgDocument29 pagesEcgSouvikDattaNo ratings yet
- Electrophysiologyofheart PDFDocument99 pagesElectrophysiologyofheart PDFsahar awaisNo ratings yet
- Interpretasi ElektrokardiografiDocument60 pagesInterpretasi ElektrokardiografiYogi GustriansyahNo ratings yet
- ALL& AML TTTDocument1 pageALL& AML TTTTsegaye HailuNo ratings yet
- Lymphatic SystemDocument10 pagesLymphatic SystemTsegaye HailuNo ratings yet
- Ans Pharmacology 01 For Pc-IDocument54 pagesAns Pharmacology 01 For Pc-ITsegaye HailuNo ratings yet
- Coagulation DisorderDocument38 pagesCoagulation DisorderTsegaye HailuNo ratings yet
- Metabolic Hemostasis MF PortionDocument68 pagesMetabolic Hemostasis MF PortionTsegaye HailuNo ratings yet
- Atherosclerosis & DyslipidemiasDocument28 pagesAtherosclerosis & DyslipidemiasTsegaye HailuNo ratings yet
- ABDOMINAL EXAMINATION EditedDocument21 pagesABDOMINAL EXAMINATION EditedTsegaye HailuNo ratings yet
- Adrenergic AntagonistsDocument44 pagesAdrenergic AntagonistsTsegaye HailuNo ratings yet
- Pathophysiology of Heart Failure - Neurohumoral Adaptations PDFDocument10 pagesPathophysiology of Heart Failure - Neurohumoral Adaptations PDFcristianamihailaNo ratings yet
- Care Plan by NCM 114Document4 pagesCare Plan by NCM 114Carmel VenezuelaNo ratings yet
- Ekg Tiara Nur AliviaDocument6 pagesEkg Tiara Nur AliviatyaraNo ratings yet
- Senam Lansia Terhadap HipertensiDocument13 pagesSenam Lansia Terhadap HipertensiHimawanNo ratings yet
- Lecture On EEg and ECGDocument46 pagesLecture On EEg and ECGAmb Waraich100% (1)
- Contemporary Perioperative Haemodynamic MonitoringDocument12 pagesContemporary Perioperative Haemodynamic MonitoringrjerezrNo ratings yet
- EKG Interpretasi Dan Lethal Aritmia: Aan NuraeniDocument34 pagesEKG Interpretasi Dan Lethal Aritmia: Aan NuraeniCitra Marchelina Novilini100% (1)
- Heart Failure in ChildrenDocument36 pagesHeart Failure in ChildrenCristinaGheorgheNo ratings yet
- Pathophysiology (Cerebrovascular Accident Hemorrhagic Right Lobe)Document4 pagesPathophysiology (Cerebrovascular Accident Hemorrhagic Right Lobe)jhonkivenNo ratings yet
- 1 s2.0 S0914508718302685 MainDocument8 pages1 s2.0 S0914508718302685 MainJose Ignacio Tarton SisimitNo ratings yet
- Dopamine HydrochlorideDocument1 pageDopamine HydrochlorideJoannes SanchezNo ratings yet
- Circulatory SystemDocument7 pagesCirculatory SystemWisdom DzombeNo ratings yet
- Respiratory Physiology: Tom Archer, MD, MBA UCSD AnesthesiaDocument81 pagesRespiratory Physiology: Tom Archer, MD, MBA UCSD AnesthesiaMirna HanintyaNo ratings yet
- Session #33 SAS - AnaPhy (Lab)Document5 pagesSession #33 SAS - AnaPhy (Lab)G INo ratings yet
- Introduction and Classification: Pathophysiology of HypertensionDocument2 pagesIntroduction and Classification: Pathophysiology of HypertensionHelen93No ratings yet
- 2020 - ESC Guidelines On Sports Cardiology and Exercise in Patients With Cardiovascular DiseaseDocument80 pages2020 - ESC Guidelines On Sports Cardiology and Exercise in Patients With Cardiovascular DiseaseHector VillamarinNo ratings yet
- Moyamoya Disease: Current Concepts and Future Perspectives: ReviewDocument11 pagesMoyamoya Disease: Current Concepts and Future Perspectives: ReviewThirumanjari KarthikeyanNo ratings yet
- Cardiohelp System Brochure-En-Non Us JapanDocument16 pagesCardiohelp System Brochure-En-Non Us JapanAnar MaharramovNo ratings yet
- Angina Pectoris Pharmacological and Acupuncture TherapyDocument5 pagesAngina Pectoris Pharmacological and Acupuncture TherapyEditor IJTSRDNo ratings yet
- Biology As Level: Practise QuestionDocument82 pagesBiology As Level: Practise QuestionTamanna AdibaNo ratings yet
- P1108 Pediatric ECG - 8feb2017Document46 pagesP1108 Pediatric ECG - 8feb2017Anonymous OY2K0XTLhuNo ratings yet