You might also like
- Clinical Nutrition Conference VisionDocument29 pagesClinical Nutrition Conference VisionMaya Rosmaria PNo ratings yet
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- History Taking Template For StudentsDocument14 pagesHistory Taking Template For Studentsx88tydcwb2No ratings yet
- Indian Female's Abdominal Pain and BreathlessnessDocument12 pagesIndian Female's Abdominal Pain and BreathlessnessayunisallehNo ratings yet
- Pedia Grand CAsEDocument33 pagesPedia Grand CAsEMichael Donn Bulic ApostolNo ratings yet
- Physical Exam and History Taking-PaedsDocument12 pagesPhysical Exam and History Taking-PaedssmexiiloriNo ratings yet
- Case Study # 1 Adult Case StudyDocument10 pagesCase Study # 1 Adult Case StudyJoam HolgadoNo ratings yet
- Community-Acquired Pneumonia (CAP)Document24 pagesCommunity-Acquired Pneumonia (CAP)Hannah HalimNo ratings yet
- Case Presentation IM DDHDocument12 pagesCase Presentation IM DDHAishwarya BharathNo ratings yet
- CMC-Preterm LaborDocument11 pagesCMC-Preterm LaborRalph AlbertoNo ratings yet
- CPC CaseDocument8 pagesCPC CasePingky khingthongNo ratings yet
- Pelamonia 24 Nov 2022Document25 pagesPelamonia 24 Nov 2022maya_rosmariaNo ratings yet
- PJT Confrence December 5th - FixDocument27 pagesPJT Confrence December 5th - Fixmaya_rosmariaNo ratings yet
- Case-Presention FinalDocument16 pagesCase-Presention Finalkristine-ann TabernaNo ratings yet
- Intracranial Lesion CaseDocument5 pagesIntracranial Lesion CasepriscaNo ratings yet
- Konfrens RS Stella Maris 5092022Document27 pagesKonfrens RS Stella Maris 5092022Maya Rosmaria PNo ratings yet
- RenalDocument11 pagesRenalayunisallehNo ratings yet
- Case Presentation CardiomyopathyDocument30 pagesCase Presentation CardiomyopathyKshayna 1234No ratings yet
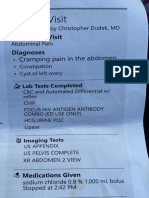
- Today's Visit: - Cramping Pain in The AbdomenDocument2 pagesToday's Visit: - Cramping Pain in The AbdomenSydney TranNo ratings yet
- Pedia HX Seizure 1Document25 pagesPedia HX Seizure 1Amer Hussein DomadoNo ratings yet
- Crohn's Disease Case StudyDocument6 pagesCrohn's Disease Case Studyjericho dinglasanNo ratings yet
- BY: Shazlin Bt. Sabaah Salwa Hanim Bt. Mohd. Saifuddin Kamarulzaman B. MuzainiDocument61 pagesBY: Shazlin Bt. Sabaah Salwa Hanim Bt. Mohd. Saifuddin Kamarulzaman B. MuzainiJohn Christopher LucesNo ratings yet
- 2017 100 Long Cases in Pediatrics Obstetrics&Gynecology Internal - Medicine-SurgeryDocument251 pages2017 100 Long Cases in Pediatrics Obstetrics&Gynecology Internal - Medicine-SurgeryAhmed Al-obariNo ratings yet
- Pleural EffusionDocument106 pagesPleural EffusionFarica Armane Aquino0% (1)
- Clinical Case: Acute Pancreatitis: Teacher: Arestegui Aguirre Diana LuzDocument13 pagesClinical Case: Acute Pancreatitis: Teacher: Arestegui Aguirre Diana LuzGrimilda PobleteNo ratings yet
- Case Write Up - Dengue FeverDocument22 pagesCase Write Up - Dengue FevervijayaNo ratings yet
- Appendicitis Signs and Symptoms GuideDocument40 pagesAppendicitis Signs and Symptoms GuideHeart TolenadaNo ratings yet
- Physical ExamDocument6 pagesPhysical ExamTroy SilverioNo ratings yet
- 1N8 Abrio, Kyra Cheyenne NicholleDocument6 pages1N8 Abrio, Kyra Cheyenne NicholleKYRA CHEYENNE NICHOLLE ABRIONo ratings yet
- Case Book Roderick FinalDocument73 pagesCase Book Roderick FinalRoderick AnthonyNo ratings yet
- Case Study 4Document22 pagesCase Study 4Angel MayNo ratings yet
- Previous LSCS Safe Delivery PlanDocument21 pagesPrevious LSCS Safe Delivery Plangokul koutikNo ratings yet
- CP3 Respiratory SystemDocument23 pagesCP3 Respiratory SystemirynNo ratings yet
- 12-Year-Old Female with RLQ Pain and Possible AppendicitisDocument4 pages12-Year-Old Female with RLQ Pain and Possible AppendicitiskymhanNo ratings yet
- Garcia, Melegrito, Zamuco: Perforated Peptic Ulcer DiseaseDocument4 pagesGarcia, Melegrito, Zamuco: Perforated Peptic Ulcer DiseasePaulo GarciaNo ratings yet
- Pregnancy Induced HypertensionDocument4 pagesPregnancy Induced HypertensionNibraz ChNo ratings yet
- Welcome TO Clinical Meeting: Presented byDocument54 pagesWelcome TO Clinical Meeting: Presented byTofayel AhmedNo ratings yet
- DANNY - RIVERA - MODIFIED VERSION - Episodic Visit TemplateDocument5 pagesDANNY - RIVERA - MODIFIED VERSION - Episodic Visit TemplateMallory ZaborNo ratings yet
- Islamic University Medical School Student Examines Elderly WomanDocument17 pagesIslamic University Medical School Student Examines Elderly WomanUsaid SulaimanNo ratings yet
- H&P For ScriptDocument12 pagesH&P For ScriptAlina KievskyNo ratings yet
- CASE PRES (Cholecystitis)Document132 pagesCASE PRES (Cholecystitis)Shelley PantinopleNo ratings yet
- Grand Conference: Clinical Clerks Openiano, Oquendo, Pasaporte, PangandianDocument65 pagesGrand Conference: Clinical Clerks Openiano, Oquendo, Pasaporte, PangandianJessa MeaNo ratings yet
- Diarrhea of 1 Day Duration: Durante, Esperon, Espino, Fernando, Figuracion, Flores, Fong, Francisco JDocument37 pagesDiarrhea of 1 Day Duration: Durante, Esperon, Espino, Fernando, Figuracion, Flores, Fong, Francisco JMisheilPascuaNo ratings yet
- Cwu Surgery Y5 AsyikinDocument21 pagesCwu Surgery Y5 AsyikinNurulasyikin MAANo ratings yet
- Patients History and Physical ExaminationDocument4 pagesPatients History and Physical Examinationeranga002No ratings yet
- Gastro 5Document1 pageGastro 5HarishNo ratings yet
- R 8Document9 pagesR 8Sadia AwanNo ratings yet
- Sample Paper Case For ClassDocument7 pagesSample Paper Case For ClassCRUZ Jill EraNo ratings yet
- IM - HX and PE TBDocument21 pagesIM - HX and PE TBTrisNo ratings yet
- Hypothyroidism DiagnosisDocument4 pagesHypothyroidism DiagnosisWan Razin Wan HassanNo ratings yet
- Konfrens IC 11 AgustusDocument26 pagesKonfrens IC 11 Agustusprimalia rosyidahNo ratings yet
- Carpio CalaycayDocument4 pagesCarpio CalaycayCzara DyNo ratings yet
- E.T.D.'s Medical History and ExamDocument8 pagesE.T.D.'s Medical History and ExamZadkiel VelasquezNo ratings yet
- Case Report V Internal MedicineDocument14 pagesCase Report V Internal MedicineGidu SaidNo ratings yet
- Case Write Up 1-CholecystitisDocument9 pagesCase Write Up 1-CholecystitisAmbhi Gana100% (1)
- Terminally Ill Child's Osteosarcoma Impact on FamilyDocument27 pagesTerminally Ill Child's Osteosarcoma Impact on FamilyRajanNo ratings yet
- Internal Medicine Case Write Up 1Document16 pagesInternal Medicine Case Write Up 1Shafiah Aqilah Mohd Jamal67% (3)
- Lung Cancer with Pleural EffusionsDocument8 pagesLung Cancer with Pleural EffusionsL4 CLERK - UY, Rhea Andrea F.No ratings yet
- Jeanne Lloraine R. Fiel Date&Time: November 23, 2020 at 5:00 P.M. Informant: Mother % Reliability: 95%Document6 pagesJeanne Lloraine R. Fiel Date&Time: November 23, 2020 at 5:00 P.M. Informant: Mother % Reliability: 95%Jeanne Lloraine FielNo ratings yet
- Ptosis and Lid RetractionDocument40 pagesPtosis and Lid Retractionsarath chandranNo ratings yet
- Aortic Aneurysm-Dr AbhishekDocument90 pagesAortic Aneurysm-Dr Abhisheksarath chandranNo ratings yet
- Plasma Cell DyscrasiasDocument68 pagesPlasma Cell Dyscrasiassarath chandranNo ratings yet
- Approach To Anemia-Iron Deficiency, Megaloblastic and Hemolytic AnemiaDocument106 pagesApproach To Anemia-Iron Deficiency, Megaloblastic and Hemolytic Anemiasarath chandranNo ratings yet
- A Powerful Graphic Liquid Crystal Display: Column #47, March 1999 by Lon GlaznerDocument16 pagesA Powerful Graphic Liquid Crystal Display: Column #47, March 1999 by Lon GlaznerVijay P PulavarthiNo ratings yet
- PH.D Scholars UGCDocument25 pagesPH.D Scholars UGCUsha MurthyNo ratings yet
- Indigo CaseDocument13 pagesIndigo Caseharsh sainiNo ratings yet
- 100-Word Replacement PDFDocument14 pages100-Word Replacement PDFTheodore Vijay100% (1)
- Diesel Pump of The Desmi GroupDocument10 pagesDiesel Pump of The Desmi Groupngocdhxd92No ratings yet
- OUM Human Anatomy Final Exam QuestionsDocument5 pagesOUM Human Anatomy Final Exam QuestionsAnandNo ratings yet
- Royal Scythians and the Slave Trade in HerodotusDocument19 pagesRoyal Scythians and the Slave Trade in HerodotusSinan SakicNo ratings yet
- EasyGreen ManualDocument33 pagesEasyGreen ManualpitoupitouNo ratings yet
- Surrealismo TriplevDocument13 pagesSurrealismo TriplevVictor LunaNo ratings yet
- Alex Tissandier Affirming Divergence PDFDocument194 pagesAlex Tissandier Affirming Divergence PDFDwi PlatomoNo ratings yet
- Si Eft Mandate FormDocument1 pageSi Eft Mandate FormdSolarianNo ratings yet
- Soil Penetrometer ManualDocument4 pagesSoil Penetrometer Manualtag_jNo ratings yet
- Business ModelsDocument10 pagesBusiness ModelsPiyushNo ratings yet
- Harsheen Kaur BhasinDocument20 pagesHarsheen Kaur Bhasincalvin kleinNo ratings yet
- Tsu m7 Practice Problems Integral CalculusDocument1 pageTsu m7 Practice Problems Integral CalculusJAMNo ratings yet
- Geraldez Vs Ca 230 Scra 329Document12 pagesGeraldez Vs Ca 230 Scra 329Cyrus Pural EboñaNo ratings yet
- What Is The Time Value of MoneyDocument6 pagesWhat Is The Time Value of MoneySadia JuiNo ratings yet
- Proposal to Enhance Science InstructionDocument4 pagesProposal to Enhance Science InstructionAzzel ArietaNo ratings yet
- Deconstuctionist CriticismDocument3 pagesDeconstuctionist CriticismStephanie PVNo ratings yet
- 2010 Christian Religious Education Past Paper - 1Document1 page2010 Christian Religious Education Past Paper - 1lixus mwangiNo ratings yet
- Samsung C&T AuditDocument104 pagesSamsung C&T AuditkevalNo ratings yet
- Major Discoveries in Science HistoryDocument7 pagesMajor Discoveries in Science HistoryRoland AbelaNo ratings yet
- Lesson Plans by Noman Niaz MaharDocument3 pagesLesson Plans by Noman Niaz MaharNoman Niaz 13No ratings yet
- How to Stop Overthinking and Make DecisionsDocument39 pagesHow to Stop Overthinking and Make DecisionsDeepak SinghNo ratings yet
- A-7 Longitudinal SectionDocument1 pageA-7 Longitudinal SectionarjayymerleNo ratings yet
- Pathways Rw1 2e U7 TestDocument9 pagesPathways Rw1 2e U7 TestGrace Ann AbanteNo ratings yet
- BATCH Bat Matrix OriginalDocument5 pagesBATCH Bat Matrix OriginalBarangay NandacanNo ratings yet
- FDP CE BroucherDocument2 pagesFDP CE BroucherAnonymous POUAc3zNo ratings yet
- Natural Gas Engines 2019Document428 pagesNatural Gas Engines 2019Паша Шадрёнкин100% (1)
- KluberDocument20 pagesKluberJako MishyNo ratings yet