You might also like
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Physical Exam and History Taking-PaedsDocument12 pagesPhysical Exam and History Taking-PaedssmexiiloriNo ratings yet
- Case-Presention FinalDocument16 pagesCase-Presention Finalkristine-ann TabernaNo ratings yet
- Obstetrics N Gynaecology MADE EASYDocument25 pagesObstetrics N Gynaecology MADE EASYAlano S. LimgasNo ratings yet
- CPC CaseDocument8 pagesCPC CasePingky khingthongNo ratings yet
- Thera 1-Case 2Document3 pagesThera 1-Case 2marih2101masrNo ratings yet
- NU 665 Pediatric Gastrointestinal Case Study - Michelle - StewardDocument10 pagesNU 665 Pediatric Gastrointestinal Case Study - Michelle - StewardMichelle StewardNo ratings yet
- FNP 2 ObesityDocument24 pagesFNP 2 Obesityapi-554096544No ratings yet
- Lower Limb WeaknessDocument15 pagesLower Limb WeaknessA MNo ratings yet
- A Woman (45 Yo) Came To An ER With Condition A Fever For 3 Days and 10 Hours BeforeDocument3 pagesA Woman (45 Yo) Came To An ER With Condition A Fever For 3 Days and 10 Hours BeforeNick BrianNo ratings yet
- HC - Issac DamianDocument10 pagesHC - Issac DamianOber SánchezNo ratings yet
- Case Write Up 1-CholecystitisDocument9 pagesCase Write Up 1-CholecystitisAmbhi Gana100% (1)
- Ward 1: Group 4: Paras, Payad, Pedrosa, Pinlac, Roldan, SalungaDocument30 pagesWard 1: Group 4: Paras, Payad, Pedrosa, Pinlac, Roldan, SalungaJoezelleNo ratings yet
- Obstetrics N Gynaecology Cases PDFDocument21 pagesObstetrics N Gynaecology Cases PDFAparna DeviNo ratings yet
- Obstetrics N Gynaecology CasesDocument21 pagesObstetrics N Gynaecology CasesMarutiNo ratings yet
- Chapter 3 SOAP NoteDocument2 pagesChapter 3 SOAP NoteKatrina Litzko50% (2)
- EM Case Write UpDocument11 pagesEM Case Write UpRaihana Rafi100% (2)
- SP Details ECE HX Taking CVS Y1Document2 pagesSP Details ECE HX Taking CVS Y1Divyaa VisvalingamNo ratings yet
- IM Gastro FinalDocument10 pagesIM Gastro FinalIzzyMaxinoNo ratings yet
- Case HistoryDocument3 pagesCase Historyapi-3747054No ratings yet
- Case Report: Tikur Anbesa Specialized HospitalDocument11 pagesCase Report: Tikur Anbesa Specialized HospitalTefera LeteboNo ratings yet
- Case Report LanaDocument20 pagesCase Report Lanaboody257No ratings yet
- Clinical Case PresentationDocument44 pagesClinical Case PresentationRUSSELL CILOTNo ratings yet
- Case 1Document5 pagesCase 1priscaNo ratings yet
- IM-Generalized Peritonitis HX PEDocument20 pagesIM-Generalized Peritonitis HX PETrisNo ratings yet
- Internal Medicine (II) 2011 LogbookDocument73 pagesInternal Medicine (II) 2011 LogbookQasim HaleimiNo ratings yet
- IVMS ICM HX Sample Write-UpDocument4 pagesIVMS ICM HX Sample Write-UpMarc Imhotep Cray, M.D.No ratings yet
- Pedia - DengueDocument10 pagesPedia - DengueJan Mikhail FrascoNo ratings yet
- Inter MykDocument4 pagesInter Mykkengeramacklina3No ratings yet
- Gyne Case PresentationDocument12 pagesGyne Case PresentationTada MinionNo ratings yet
- Case 1Document3 pagesCase 1איתי עוזרNo ratings yet
- Deipan Arjunan - 20UMB03886 - CWU 2 - IM Group 1Document30 pagesDeipan Arjunan - 20UMB03886 - CWU 2 - IM Group 1Deipan ArjunanNo ratings yet
- Safari - Jul 27, 2019 at 7:12 AMDocument1 pageSafari - Jul 27, 2019 at 7:12 AMKo NgeNo ratings yet
- Cadisal MW 1ST Week RequiementsDocument36 pagesCadisal MW 1ST Week RequiementsJonathan GonzalesNo ratings yet
- Case Report V Internal MedicineDocument14 pagesCase Report V Internal MedicineGidu SaidNo ratings yet
- n703 Chronic Soap NoteDocument3 pagesn703 Chronic Soap NoteJeffrey ViernesNo ratings yet
- Comment (1) : Comment (2) :: DemographicsDocument2 pagesComment (1) : Comment (2) :: DemographicsCatNo ratings yet
- Prepared By: Sarra'a Fawaz AbbasDocument36 pagesPrepared By: Sarra'a Fawaz AbbasSarraa NajimNo ratings yet
- Uro 1Document2 pagesUro 1HarishNo ratings yet
- Case Base DiscussionDocument19 pagesCase Base DiscussionNu JoeNo ratings yet
- CWU - AnaestiologyDocument8 pagesCWU - AnaestiologyAmbhi GanaNo ratings yet
- Case StudyDocument3 pagesCase StudyD A M N E R ANo ratings yet
- Stroke - Final ReportDocument16 pagesStroke - Final ReportgolokipokNo ratings yet
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloDocument15 pagesCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisNo ratings yet
- Patients History and Physical ExaminationDocument4 pagesPatients History and Physical Examinationeranga002No ratings yet
- Tehnik Penyusunan StatusDocument7 pagesTehnik Penyusunan StatusShelly Stephanie BintoroNo ratings yet
- Week 4 - Day 1 - Sample History and Physical Exam Write-UpDocument5 pagesWeek 4 - Day 1 - Sample History and Physical Exam Write-UpNsikan GabrielNo ratings yet
- Neuroblastoma Dr. Rapp 5.17.2013Document14 pagesNeuroblastoma Dr. Rapp 5.17.2013Emily EresumaNo ratings yet
- Obstetric and Gynacology CasesDocument51 pagesObstetric and Gynacology CasesElly PetroNo ratings yet
- Case No 7Document7 pagesCase No 7Sameena .jNo ratings yet
- Anaemia in PregnancyDocument29 pagesAnaemia in PregnancySampritha P GNo ratings yet
- Surgery Case Write Up UGIHDocument37 pagesSurgery Case Write Up UGIHRahul Audenesen33% (3)
- 3 HPLCDocument9 pages3 HPLClorrainebarandonNo ratings yet
- Antanatal Care PlanDocument12 pagesAntanatal Care PlanmohildasadiaNo ratings yet
- Case Study About Skin DiseasesDocument7 pagesCase Study About Skin DiseasesSameena .jNo ratings yet
- Sample Write UpDocument2 pagesSample Write UpNar Patrick Padilla100% (1)
- Pedia Case For Group 2Document5 pagesPedia Case For Group 2Ann Mariz DominguezNo ratings yet
- Case Study About Valvular DiseaseDocument6 pagesCase Study About Valvular DiseaseSameena .jNo ratings yet
- Sem 4 OBGYNPresentationDocument16 pagesSem 4 OBGYNPresentationAdamNo ratings yet
- FAO Fish Handbook Fish FarmingDocument89 pagesFAO Fish Handbook Fish FarmingLee kamunya100% (1)
- Connection DesignDocument33 pagesConnection Designjesus curielNo ratings yet
- API 510 Study GuideDocument3 pagesAPI 510 Study GuidedanikakaNo ratings yet
- L23Document29 pagesL23Mary MorseNo ratings yet
- Amp-Eng Anger Management ProfileDocument6 pagesAmp-Eng Anger Management Profileminodora100% (1)
- Physical, Biology and Chemical Environment: Its Effect On Ecology and Human HealthDocument24 pagesPhysical, Biology and Chemical Environment: Its Effect On Ecology and Human Health0395No ratings yet
- Nexgard For Dogs and Puppies Free 2 Day ShippingDocument1 pageNexgard For Dogs and Puppies Free 2 Day Shippinglyly23748No ratings yet
- (Nikolaj Wolfson, Alexander Lerner, Leonid Roshal (B-Ok - CC)Document589 pages(Nikolaj Wolfson, Alexander Lerner, Leonid Roshal (B-Ok - CC)Andi sutandi100% (1)
- Fawwaz Muhammad X-Ipa 1: 1. Who Is The Main Character of The Story? 2. When Did It Happen?Document3 pagesFawwaz Muhammad X-Ipa 1: 1. Who Is The Main Character of The Story? 2. When Did It Happen?Abbas AminuNo ratings yet
- Rudi Tampubolon - Risk Management ProcessDocument21 pagesRudi Tampubolon - Risk Management ProcessSeptian WisudaniNo ratings yet
- IWGIA Book The Indigenous World 2021 ENGDocument824 pagesIWGIA Book The Indigenous World 2021 ENGREy FOxNo ratings yet
- Colorful Grade 1 Writing Practice English WorksheetDocument9 pagesColorful Grade 1 Writing Practice English WorksheetLeoni Franc100% (1)
- Arduino CertificationDocument8 pagesArduino Certificationhack reportNo ratings yet
- Aaos PDFDocument4 pagesAaos PDFWisnu CahyoNo ratings yet
- Bio 2Document3 pagesBio 2ganchimeg gankhuuNo ratings yet
- Department of Civil Engineering Uttara University: LaboratoryDocument102 pagesDepartment of Civil Engineering Uttara University: LaboratorytaniaNo ratings yet
- New Approaches To Cryopreservation of Cells, Tissues, and OrgansDocument19 pagesNew Approaches To Cryopreservation of Cells, Tissues, and OrgansLaura CursaruNo ratings yet
- Escape From The Western Diet Summary RevisedDocument3 pagesEscape From The Western Diet Summary Revisedapi-385530863100% (1)
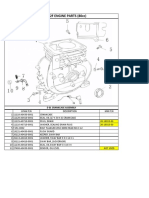
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- Multiple Choice Questions: Topic Covered Are As FollowsDocument3 pagesMultiple Choice Questions: Topic Covered Are As FollowsBikash SahuNo ratings yet
- Unit 1 Marks: 15 Introduction To Micro System and Smart SystemsDocument9 pagesUnit 1 Marks: 15 Introduction To Micro System and Smart SystemsSudarsh KNo ratings yet
- Zinc Silicate or Zinc Epoxy As The Preferred High Performance PrimerDocument10 pagesZinc Silicate or Zinc Epoxy As The Preferred High Performance Primerbabis1980100% (1)
- HY Endocrine UsmleDocument22 pagesHY Endocrine UsmleNakhal JararNo ratings yet
- 94 175 1 SM PDFDocument8 pages94 175 1 SM PDFikaNo ratings yet
- MSC Nursing Approved Thesis Topics 2009-12Document32 pagesMSC Nursing Approved Thesis Topics 2009-12Anonymous 4L20Vx60% (5)
- Benefits of Playing Badminton (An Essay)Document2 pagesBenefits of Playing Badminton (An Essay)Haryoung Sta CruzNo ratings yet
- Current Issues On Construction Project ManagementDocument2 pagesCurrent Issues On Construction Project ManagementJoyce Abegail De PedroNo ratings yet
- Pharmacology: Jump To Navigation Jump To SearchDocument18 pagesPharmacology: Jump To Navigation Jump To SearchJennie KimNo ratings yet
- ACS AMI FacilitatorDocument21 pagesACS AMI FacilitatorPaul Zantua57% (7)
- PT3 Practices EssayDocument61 pagesPT3 Practices EssayGolden Fingers100% (3)