You might also like
- ADHD In Adults: Am I ADHD? Interactive Questions For ADHD Assessment: Learn If You Suffer From ADHD - Take This Assessment TestFrom EverandADHD In Adults: Am I ADHD? Interactive Questions For ADHD Assessment: Learn If You Suffer From ADHD - Take This Assessment TestNo ratings yet
- OPPOSITIONAL DEFIANT DISORDER: Understanding, Managing, and Thriving with Oppositional Defiant Disorder (2024 Guide for Beginners)From EverandOPPOSITIONAL DEFIANT DISORDER: Understanding, Managing, and Thriving with Oppositional Defiant Disorder (2024 Guide for Beginners)No ratings yet
- Disorders of ChildhoodDocument61 pagesDisorders of ChildhoodEdom TesfayeNo ratings yet
- Child DisordersDocument111 pagesChild Disorderspriyanka rajNo ratings yet
- Disruptive Impulse Control & Conduct DisorderDocument31 pagesDisruptive Impulse Control & Conduct Disorder-sparkle1234100% (1)
- Disruptive Behaviour Disorders: Donna Dowling Child & Adolescent Psychiatrist Townsville CAYASDocument76 pagesDisruptive Behaviour Disorders: Donna Dowling Child & Adolescent Psychiatrist Townsville CAYASVukashin.meNo ratings yet
- Psychiatric Disorders in Childhood and AdolescenceDocument81 pagesPsychiatric Disorders in Childhood and Adolescenceabriham100% (1)
- Disorders Usually 1 Diagnosed in Infancy, Childhood, & AdolescenceDocument31 pagesDisorders Usually 1 Diagnosed in Infancy, Childhood, & AdolescenceShahzad Bashir ShamsNo ratings yet
- Behavioural Disorders (1)Document41 pagesBehavioural Disorders (1)samadrita dasNo ratings yet
- Conduct Disorder: Welcome To The PresentationDocument34 pagesConduct Disorder: Welcome To The PresentationalaminNo ratings yet
- Child Psychiatry: ADHD, Conduct Disorder, Emotional Disorder, Elimination DisorderDocument53 pagesChild Psychiatry: ADHD, Conduct Disorder, Emotional Disorder, Elimination DisorderCodillia CheongNo ratings yet
- 9-Child and Adolescent PsychiatryDocument32 pages9-Child and Adolescent PsychiatryZ26No ratings yet
- Children and Youth With Behavioural ProblemsDocument25 pagesChildren and Youth With Behavioural ProblemsSidhi YadavNo ratings yet
- Signs of ADHD, Diagnosis and Differential DiagnosisDocument25 pagesSigns of ADHD, Diagnosis and Differential DiagnosisYasNo ratings yet
- Understanding Disruptive Behaviours in Children with Autism Spectrum DisordersDocument54 pagesUnderstanding Disruptive Behaviours in Children with Autism Spectrum Disordersman_sengalNo ratings yet
- Child and Adolescent DisordersDocument49 pagesChild and Adolescent DisordersKirsten Padilla ChuaNo ratings yet
- Oppositional Defiant Disorder OddDocument10 pagesOppositional Defiant Disorder Oddapi-360330020No ratings yet
- ADHD PresentationDocument21 pagesADHD PresentationZainab Ali HassanNo ratings yet
- Psychiatric Disorders in Childhood and AdolescenceDocument81 pagesPsychiatric Disorders in Childhood and AdolescenceDhartie FweshBoy NasifNo ratings yet
- Conduct Disorder AladejareDocument44 pagesConduct Disorder AladejareSamuel AladejareNo ratings yet
- IT 5 - Gangguan Perkembangan Pervasif (ADHD) - RISDocument15 pagesIT 5 - Gangguan Perkembangan Pervasif (ADHD) - RISIqbal HabibieNo ratings yet
- What Parents and Teachers Should Know About Adhd: Center For Children and FamiliesDocument2 pagesWhat Parents and Teachers Should Know About Adhd: Center For Children and FamiliesWhisperer BowenNo ratings yet
- D.2 Odd 2018Document24 pagesD.2 Odd 2018Kibru le EyesusNo ratings yet
- Conduct DisorderDocument26 pagesConduct DisorderArabelle GO100% (1)
- Autism Spectrum Disorder With Videos 2022 - FAYDocument26 pagesAutism Spectrum Disorder With Videos 2022 - FAYNikky SilvestreNo ratings yet
- Attention Deficit Hyperactivity Disorder in Children & AdolescentsDocument68 pagesAttention Deficit Hyperactivity Disorder in Children & AdolescentsSiva KumarrNo ratings yet
- Childhood and Adolescent DisorderDocument54 pagesChildhood and Adolescent DisorderRiccyNo ratings yet
- Attention Deficit Hyperactivity Disorder (ADHD)Document47 pagesAttention Deficit Hyperactivity Disorder (ADHD)HarisSafiNo ratings yet
- Psyc 302 Week 10 Childhood AgingDocument54 pagesPsyc 302 Week 10 Childhood AgingENo ratings yet
- Understanding Disruptive Behavior DisordersDocument46 pagesUnderstanding Disruptive Behavior DisordersManisha100% (4)
- Childhood Emotional Disorders: Treatments and Interventions for NursesDocument28 pagesChildhood Emotional Disorders: Treatments and Interventions for NursesjoycechicagoNo ratings yet
- III. Disorders Diagnosed in Infancy, Childhood, And Adolescence (1)Document13 pagesIII. Disorders Diagnosed in Infancy, Childhood, And Adolescence (1)Dominic RomanillosNo ratings yet
- Attention Deficit Hyperactivity DisorderDocument42 pagesAttention Deficit Hyperactivity DisordermengakuNo ratings yet
- IntroductionDocument3 pagesIntroductionFatima ZahraNo ratings yet
- Oppositional Defiant DisorderDocument6 pagesOppositional Defiant DisorderTiara YunitasariNo ratings yet
- Adolescent Disruptive BehaviourDocument15 pagesAdolescent Disruptive BehaviourLavanya PNo ratings yet
- ADHDDocument21 pagesADHDYuniita VerayantiiNo ratings yet
- Neuro Developmental DisordersDocument59 pagesNeuro Developmental Disorderskgaseitsiwe0952No ratings yet
- Asd and Adhd (Week 16)Document57 pagesAsd and Adhd (Week 16)Krisha Mabel TabijeNo ratings yet
- Management of Mental Disorder in AdolescentDocument20 pagesManagement of Mental Disorder in AdolescentMuhammad mukramNo ratings yet
- Attention Deficit Hyperactivity Disorder - ADHDDocument21 pagesAttention Deficit Hyperactivity Disorder - ADHDFrancis A. BuenaventuraNo ratings yet
- Diagnosing Assessing Learners With Adhd and Gifted G 4Document78 pagesDiagnosing Assessing Learners With Adhd and Gifted G 4Oliver A. DuyuconNo ratings yet
- Oppositional Defiant DisorderDocument14 pagesOppositional Defiant DisorderKaren ComiaNo ratings yet
- ADHD PowerPointDocument33 pagesADHD PowerPointF. HammoudNo ratings yet
- W6L28Document16 pagesW6L28N SinghNo ratings yet
- Developmental Disorder 4 TH YearDocument32 pagesDevelopmental Disorder 4 TH YearPraneethaNo ratings yet
- Child Psychopathology - Student VersionDocument42 pagesChild Psychopathology - Student VersionEmma KornatowskiNo ratings yet
- Faktor Dan Deteksi Dini Masalah Kejiwaan RemajaDocument54 pagesFaktor Dan Deteksi Dini Masalah Kejiwaan RemajaputriluftiNo ratings yet
- Attention Deficits Hyperactivity Disorder (Adhd)Document7 pagesAttention Deficits Hyperactivity Disorder (Adhd)Catherine LaraNo ratings yet
- Understanding and Diagnosing ADHDDocument39 pagesUnderstanding and Diagnosing ADHDPtrc Lbr LpNo ratings yet
- E.3 DMDD 2017Document17 pagesE.3 DMDD 2017Maria Helena Pedraza MNo ratings yet
- Common Child Psychiatric DisordersDocument30 pagesCommon Child Psychiatric DisordersabrihamNo ratings yet
- AutismDocument34 pagesAutismDianne Rose AgliamNo ratings yet
- Disruptive Behavior of childhoodDocument31 pagesDisruptive Behavior of childhoodabdulghaniNo ratings yet
- Children With Special Needs PresentationDocument50 pagesChildren With Special Needs PresentationMarcela Mora Espinoza50% (2)
- Child and Adolescent DisordersDocument32 pagesChild and Adolescent Disorderscubezero100% (1)
- Adhd 1Document11 pagesAdhd 1Hooria AmerNo ratings yet
- Behavioural DisordersDocument9 pagesBehavioural DisordersEsther OmokanjuNo ratings yet
- Externalizing BehaviorsDocument45 pagesExternalizing BehaviorstrayNo ratings yet
- Faktor dan Deteksi Dini Masalah Jiwa RemajaDocument54 pagesFaktor dan Deteksi Dini Masalah Jiwa RemajaYauffa Hanna Elt MisykahNo ratings yet
- Fault Code 498 Engine Oil Level Sensor Circuit - Voltage Above Normal, or Shorted To High SourceDocument13 pagesFault Code 498 Engine Oil Level Sensor Circuit - Voltage Above Normal, or Shorted To High SourceAhmedmah100% (1)
- 8.4.3 Alien Genetics LabDocument2 pages8.4.3 Alien Genetics LabCharles KnightNo ratings yet
- Perpus Pusat Bab 1 Dan 2Document62 pagesPerpus Pusat Bab 1 Dan 2imam rafifNo ratings yet
- SP-1127 - Layout of Plant Equipment and FacilitiesDocument11 pagesSP-1127 - Layout of Plant Equipment and FacilitiesParag Lalit SoniNo ratings yet
- Advanced Software Upgrade GuideDocument5 pagesAdvanced Software Upgrade GuideMiguel RibeiroNo ratings yet
- Laboratory Exercise Set #10 Printers General Instructions:: Lab 11.1 Backing Up An Ios Device To A PC or Mac Using ItunesDocument29 pagesLaboratory Exercise Set #10 Printers General Instructions:: Lab 11.1 Backing Up An Ios Device To A PC or Mac Using ItunesSam MadroneroNo ratings yet
- Human Persons Are Oriented Toward Their Impending DeathDocument40 pagesHuman Persons Are Oriented Toward Their Impending DeathNaddy Retxed100% (1)
- Buck 1948Document9 pagesBuck 1948Carlos Mora100% (1)
- Centrifugal PumpDocument44 pagesCentrifugal PumpAmishaan KharbandaNo ratings yet
- Underplate GroutingDocument1 pageUnderplate GroutingminedataNo ratings yet
- AlumaCore OPGWDocument1 pageAlumaCore OPGWlepouletNo ratings yet
- BU - Assignment 2 PDFDocument2 pagesBU - Assignment 2 PDFMaliha FarzanaNo ratings yet
- 01 LANG Forgiarini Low Energy EmulsificationDocument8 pages01 LANG Forgiarini Low Energy EmulsificationDuvánE.DueñasLópezNo ratings yet
- Lecture Notes (Chapter 2.3 Triple Integral)Document5 pagesLecture Notes (Chapter 2.3 Triple Integral)shinee_jayasila2080100% (1)
- Laser Light PriceDocument5 pagesLaser Light Priceluis palominoNo ratings yet
- Understanding Negation in Indian LogicDocument10 pagesUnderstanding Negation in Indian LogicvasubandhuNo ratings yet
- Solving Systems of Linear Equations in Two VariablesDocument13 pagesSolving Systems of Linear Equations in Two VariablesMarie Tamondong50% (2)
- Part IIDocument281 pagesPart IILeng SovannarithNo ratings yet
- Design of Base Slab of UGTDocument5 pagesDesign of Base Slab of UGTAamir SuhailNo ratings yet
- Hydrology Notes 4 PDFDocument12 pagesHydrology Notes 4 PDFSudin PradhanNo ratings yet
- Spreadsheet Practice Exercises-2017Document43 pagesSpreadsheet Practice Exercises-2017Sur Velan100% (1)
- Organization Management and LeadershipDocument26 pagesOrganization Management and LeadershipOtilia BadeaNo ratings yet
- Profile Shakeel Carpentry Joinery WorksDocument46 pagesProfile Shakeel Carpentry Joinery WorksShakeel Ahmad100% (1)
- Sub Net Questions With AnsDocument5 pagesSub Net Questions With AnsSavior Wai Hung WongNo ratings yet
- LP Fuel Gas SystemDocument6 pagesLP Fuel Gas SystemAnonymous QSfDsVxjZNo ratings yet
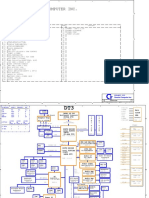
- Acer Aspire 1710 (Quanta DT3) PDFDocument35 pagesAcer Aspire 1710 (Quanta DT3) PDFMustafa AkanNo ratings yet
- 16656561931665656193FinancialModellingProfessional 1 (1) CompressedDocument17 pages16656561931665656193FinancialModellingProfessional 1 (1) CompressedDharmik UndaviyaNo ratings yet
- Ddec IV Application and InstallationDocument148 pagesDdec IV Application and Installationsptecnico8292% (36)
- ASTM C1019 GroutingDocument4 pagesASTM C1019 GroutingTrung Hieu NguyenNo ratings yet
- 2022 AMC Paper MP OMRDocument12 pages2022 AMC Paper MP OMRshilpa_aryan100% (1)