You might also like
- Ancient Remedies - DR Josh AxeDocument424 pagesAncient Remedies - DR Josh AxeLinh Nguyen100% (13)
- Causes of Speech DisordersDocument23 pagesCauses of Speech DisordersNitya100% (1)
- Cough: Adilah: PhysiotherapistDocument19 pagesCough: Adilah: PhysiotherapistAleen ZakiNo ratings yet
- List of Medical Mnemonics - WikipediaDocument60 pagesList of Medical Mnemonics - WikipediaAmir ShedNo ratings yet
- Seminar On CV Thoracic SurgeriesDocument81 pagesSeminar On CV Thoracic SurgeriesMegha lakraNo ratings yet
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeFrom EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeNo ratings yet
- Handbook of Surgical Care For House OfficersDocument22 pagesHandbook of Surgical Care For House OfficersDeep SleepNo ratings yet
- Heal Yourself Naturally PaidalajinDocument219 pagesHeal Yourself Naturally Paidalajinluis alejandro osorio100% (7)
- Lesson Plan Pulmonary TuberculosisDocument16 pagesLesson Plan Pulmonary TuberculosisKatherine 'Chingboo' Leonico Laud82% (22)
- Tuberculous Peritonitis:what About Imaging: Poster No.: Congress: Type: AuthorsDocument9 pagesTuberculous Peritonitis:what About Imaging: Poster No.: Congress: Type: AuthorswurifreshNo ratings yet
- CT Finding in Acute PeritonitisDocument16 pagesCT Finding in Acute Peritonitisyossy aciNo ratings yet
- Peritoneal Tuberculosis Mimiking Gastrointestinal Stromal TumorDocument3 pagesPeritoneal Tuberculosis Mimiking Gastrointestinal Stromal TumorIJAR JOURNALNo ratings yet
- Laparoscopy and Primary Diffuse MalignantDocument5 pagesLaparoscopy and Primary Diffuse Malignantmalvina.sekolonik911No ratings yet
- Small Intestine TumorsDocument8 pagesSmall Intestine TumorspkotaphcNo ratings yet
- Choledochal Cysts: Part 2 of 3: DiagnosisDocument6 pagesCholedochal Cysts: Part 2 of 3: DiagnosisKarla ChpNo ratings yet
- Abd TBReviewDocument4 pagesAbd TBReviewdrelvNo ratings yet
- Abdominal TB 2Document4 pagesAbdominal TB 2Yousra AhmedNo ratings yet
- Horton, K. M., Corl, F. M., & Fishman, E. K. (2000) - CT Evaluation of The Colon - Inflammatory Disease. RadioGraphics, 20 (2), 399-418Document20 pagesHorton, K. M., Corl, F. M., & Fishman, E. K. (2000) - CT Evaluation of The Colon - Inflammatory Disease. RadioGraphics, 20 (2), 399-418PauloCostaNo ratings yet
- Cistita Glandulo Chistica - Caz ClinicDocument3 pagesCistita Glandulo Chistica - Caz ClinicBarbuta AlexandraNo ratings yet
- Obstruccion Intestinal MalignaDocument11 pagesObstruccion Intestinal MalignaMaria Del PilarNo ratings yet
- Ultrasonography of The Liver and Spleen in Brazilian Patients With Hepatosplenic Schistosomiasis and CirrhosisDocument4 pagesUltrasonography of The Liver and Spleen in Brazilian Patients With Hepatosplenic Schistosomiasis and CirrhosisdenisegmeloNo ratings yet
- Primary Pure Squamous Cell Carcinoma of The Duodenum: A Case ReportDocument4 pagesPrimary Pure Squamous Cell Carcinoma of The Duodenum: A Case ReportGeorge CiorogarNo ratings yet
- Peritoneal Tuberculosis: ReviewDocument5 pagesPeritoneal Tuberculosis: ReviewEvellyna MeilanyNo ratings yet
- GRP2016 5623718Document10 pagesGRP2016 5623718erikafebriyanarNo ratings yet
- Aghiz 3Document12 pagesAghiz 3nandaaa aprilNo ratings yet
- cLINICAL PRACTICE GUIDELINESDocument7 pagescLINICAL PRACTICE GUIDELINESdrmolinammNo ratings yet
- AIDS CholangiopathyDocument7 pagesAIDS CholangiopathyedwincliffordNo ratings yet
- Accuracy of Ultrasonography in The Diagnosis of Acute Calculous Cholecystitis: Review of The LiteratureDocument4 pagesAccuracy of Ultrasonography in The Diagnosis of Acute Calculous Cholecystitis: Review of The LiteratureAnasriNstNo ratings yet
- Distinguishing Tuberculosis and Crohn's Disease in Developing Countries: How Certain Can You Be of The Diagnosis?Document5 pagesDistinguishing Tuberculosis and Crohn's Disease in Developing Countries: How Certain Can You Be of The Diagnosis?Naja HasnandaNo ratings yet
- 29051-Texto Do Trabalho-123037-2-10-20221229Document3 pages29051-Texto Do Trabalho-123037-2-10-20221229Luis Curvo SemedoNo ratings yet
- CL 5Document7 pagesCL 5ninaindriyaninNo ratings yet
- Css CT Scan AbdomenDocument54 pagesCss CT Scan AbdomenUlfa DiyaNo ratings yet
- Klatskin TumorsDocument21 pagesKlatskin TumorsCristi ZamfirNo ratings yet
- July 1991 B PDFDocument4 pagesJuly 1991 B PDFRhenofkunair0% (1)
- Manuscript Info: International Journal of Advanced ResearchDocument5 pagesManuscript Info: International Journal of Advanced Researchadil2050No ratings yet
- Management of Pseudomyxoma Peritonei: Review ArticleDocument9 pagesManagement of Pseudomyxoma Peritonei: Review ArticleTee VillanuevaNo ratings yet
- Bladder NCCNDocument17 pagesBladder NCCNJoriza TamayoNo ratings yet
- Malignant Pleural MesotheliomaDocument14 pagesMalignant Pleural MesotheliomaIulyaNo ratings yet
- Indications of Cholecystectomy in Gallstone DiseaseDocument6 pagesIndications of Cholecystectomy in Gallstone DiseaseTovan PerinandikaNo ratings yet
- Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy For Pseudomyxoma Peritonei in A Liver-Transplanted Patient: A Case ReportDocument5 pagesCytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy For Pseudomyxoma Peritonei in A Liver-Transplanted Patient: A Case Reportyerich septaNo ratings yet
- Peritoneal TB.Document5 pagesPeritoneal TB.Hanny FadhilaNo ratings yet
- Nephroblastoma: Radiological and Pathological Diagnosis of A Case With Liver MetastasesDocument5 pagesNephroblastoma: Radiological and Pathological Diagnosis of A Case With Liver MetastasesfifahcantikNo ratings yet
- Weber 2015Document12 pagesWeber 2015Nikos SerifisNo ratings yet
- 2019-Urinary Tract CytologyDocument14 pages2019-Urinary Tract CytologyLucas Da SilvaNo ratings yet
- Pombo 1998Document4 pagesPombo 1998Viviana MartínezNo ratings yet
- Aproximación Multidisciplinaria Al Diagnóstico y Tratamiento de La Obs Intestinal 2018Document124 pagesAproximación Multidisciplinaria Al Diagnóstico y Tratamiento de La Obs Intestinal 2018Jorge Nuñez LucicNo ratings yet
- Acute and Chronic in Ammation of The Biliary SystemDocument4 pagesAcute and Chronic in Ammation of The Biliary Systemfawzan mohammadNo ratings yet
- Carcinoma of The OesophagusDocument27 pagesCarcinoma of The Oesophagusmomodou s jallowNo ratings yet
- Abdomen Agudo - Radiologic Clinics of Northamerica 2003Document254 pagesAbdomen Agudo - Radiologic Clinics of Northamerica 2003arsilbNo ratings yet
- Pertanyaan Referat CA SigmoidDocument9 pagesPertanyaan Referat CA SigmoidBelladinaMMNo ratings yet
- Sindrom Deimons MeigsDocument7 pagesSindrom Deimons MeigsTudor TudorgNo ratings yet
- CT Peritoneal Carcinomat and Mimics 2014Document12 pagesCT Peritoneal Carcinomat and Mimics 2014gatoflacoNo ratings yet
- Imaging For InflammatoryDocument16 pagesImaging For InflammatoryJEFFERSON MUÑOZNo ratings yet
- The Role of Imaging in Inflammatory Bowel Disease EvaluationDocument15 pagesThe Role of Imaging in Inflammatory Bowel Disease Evaluationafudaru6043No ratings yet
- Trichobezoar With Large Bowel Obstruction in Children - Case ReportDocument3 pagesTrichobezoar With Large Bowel Obstruction in Children - Case ReportSajag GuptaNo ratings yet
- IJRP 100931120222804 (1) - CompressedDocument7 pagesIJRP 100931120222804 (1) - CompressedKlinik Bpjs AthariNo ratings yet
- (2020) Colonography Evaluation of The Relationship Between Colon Anatomy and DiverticulaDocument7 pages(2020) Colonography Evaluation of The Relationship Between Colon Anatomy and DiverticulaChristian ToalongoNo ratings yet
- Atika RozaliDocument15 pagesAtika Rozaliatika rozaliaNo ratings yet
- Pancreas Cyst: Eric Trawick Eus Conference J U N E 2 0 1 1Document26 pagesPancreas Cyst: Eric Trawick Eus Conference J U N E 2 0 1 1Dipika JangpangiNo ratings yet
- Idiopathic Sclerosing Encapsulating Peritonitis: Abdominal CocoonDocument6 pagesIdiopathic Sclerosing Encapsulating Peritonitis: Abdominal CocoonRameshKumarNo ratings yet
- 48 Devadass EtalDocument4 pages48 Devadass EtaleditorijmrhsNo ratings yet
- Ecografía ProstaticaDocument9 pagesEcografía ProstaticadynachNo ratings yet
- 180007-Article Text-459426-1-10-20181123Document5 pages180007-Article Text-459426-1-10-20181123OB-GYNE DEPARTMENTNo ratings yet
- Obstructive Jaundice Aetiological SpectrDocument8 pagesObstructive Jaundice Aetiological Spectrvvwaghmare30No ratings yet
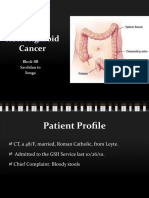
- Rectosigmoid Cancer: Block 8B Sacdalan To SengaDocument58 pagesRectosigmoid Cancer: Block 8B Sacdalan To SengaAngeli-Tristel SaquitanNo ratings yet
- Amjcaserep 21 E920438Document5 pagesAmjcaserep 21 E920438afifahNo ratings yet
- CT Findings in Acute Peritonitis: A Pattern-Based ApproachDocument6 pagesCT Findings in Acute Peritonitis: A Pattern-Based ApproachNia FitriyaniNo ratings yet
- Colorectal Cancer Liver Metastases: A Comprehensive Guide to ManagementFrom EverandColorectal Cancer Liver Metastases: A Comprehensive Guide to ManagementMauro Monteiro CorreiaNo ratings yet
- PR 31.7.22Document21 pagesPR 31.7.22Intan EklesianaNo ratings yet
- PR 21.07.22Document1 pagePR 21.07.22Intan EklesianaNo ratings yet
- Bahan Trauma AnakDocument12 pagesBahan Trauma AnakIntan EklesianaNo ratings yet
- ArdsDocument1 pageArdsIntan EklesianaNo ratings yet
- Dental Conditions in Patients With Bipolar Disorder On Long-Term Lithium Maintenance TherapyDocument4 pagesDental Conditions in Patients With Bipolar Disorder On Long-Term Lithium Maintenance TherapyCosminNo ratings yet
- 9699_PHE_2016_Complete_Immunisation_Schedule_SUMMER16_A4_16Document2 pages9699_PHE_2016_Complete_Immunisation_Schedule_SUMMER16_A4_16Sagar LodhiaNo ratings yet
- Splenectomy VaccinesDocument4 pagesSplenectomy VaccinesameliaNo ratings yet
- The World PandemicDocument3 pagesThe World PandemicMariel Niña ErasmoNo ratings yet
- Chap 14 Micropara ReviewerDocument25 pagesChap 14 Micropara RevieweryanNo ratings yet
- Prevention and Control of Infectious Diseases Act - Act 342Document32 pagesPrevention and Control of Infectious Diseases Act - Act 342appakhabarNo ratings yet
- Clinical Practice Guidelines For Management of Bipolar DisorderDocument16 pagesClinical Practice Guidelines For Management of Bipolar DisorderKavita kumariNo ratings yet
- Postpartum Purulent-Septic Diseases (Peritonitis, Sepsis, Toxic-Infectious Shock)Document64 pagesPostpartum Purulent-Septic Diseases (Peritonitis, Sepsis, Toxic-Infectious Shock)Muhammed ElnakibNo ratings yet
- Physical Medicine Amp RehabilitationDocument1 pagePhysical Medicine Amp RehabilitationH SHABANANo ratings yet
- Week 4 Ha Rle Post Test Answer KeyDocument5 pagesWeek 4 Ha Rle Post Test Answer KeyDanelyn PerezNo ratings yet
- B.inggris Covid 19 DimassDocument3 pagesB.inggris Covid 19 DimassDimas frasetyoNo ratings yet
- Diseases of The StomachDocument59 pagesDiseases of The StomachElvisNo ratings yet
- World Hearing DayDocument27 pagesWorld Hearing DayPomy AgrawalNo ratings yet
- Management of Advanced Peritonitis PP TDocument106 pagesManagement of Advanced Peritonitis PP Tvedant kanadeNo ratings yet
- Nle FC Manila 2023 May - EDITEDDocument12 pagesNle FC Manila 2023 May - EDITEDAngela NeriNo ratings yet
- Infection Basics: Biology 4310 Virology Spring 2020Document49 pagesInfection Basics: Biology 4310 Virology Spring 2020Robin SinghNo ratings yet
- Abnormal Psychology: Historical and Modern Perspectives: Total Assessment Guide (T.A.G.)Document29 pagesAbnormal Psychology: Historical and Modern Perspectives: Total Assessment Guide (T.A.G.)Rachelle SalcedoNo ratings yet
- Image Production and Evaluation: Radiographic ContrastDocument30 pagesImage Production and Evaluation: Radiographic ContrastLyht TVNo ratings yet
- Abnormal Psychology Chapter 2 (Barlow) : Multidimensional Integrative ApproachDocument6 pagesAbnormal Psychology Chapter 2 (Barlow) : Multidimensional Integrative ApproachWill BendijoNo ratings yet
- Emerg Med Clin North Am 2024 Feb 42 (1) 41-52Document12 pagesEmerg Med Clin North Am 2024 Feb 42 (1) 41-52arturo92marinNo ratings yet
- Uterine FibroidsDocument46 pagesUterine FibroidsRavindranatha AnNo ratings yet
- Jamu Herb Guide Info On Individual HerbsDocument4 pagesJamu Herb Guide Info On Individual HerbsLinda PrideNo ratings yet