You might also like
- HivDocument29 pagesHivSUTHAN100% (2)
- Treating Hoarding in Midlife and Older AdultsDocument101 pagesTreating Hoarding in Midlife and Older Adultsrgr4321100% (2)
- Career Test High School College Students Free Job Quiz Best TestsDocument2 pagesCareer Test High School College Students Free Job Quiz Best TestsShibaQLeapNo ratings yet
- Pleural Effusion - ClinicalKeyDocument13 pagesPleural Effusion - ClinicalKeyWialda Dwi rodyahNo ratings yet
- Donating Blood Saves LivesDocument4 pagesDonating Blood Saves LivesGigi2000100% (2)
- NBHS1112 Biochemistry/ Biokimia May Semester 2022Document16 pagesNBHS1112 Biochemistry/ Biokimia May Semester 2022amu tha100% (1)
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- Hepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetDocument48 pagesHepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetNurhidayahNo ratings yet
- Pharmacy Technician Course Review and Paper PatternDocument16 pagesPharmacy Technician Course Review and Paper PatternRphTehniat ZahraNo ratings yet
- Understanding Male Genitourinary CancersDocument7 pagesUnderstanding Male Genitourinary CancersWoo Rin ParkNo ratings yet
- Mollison's Blood Transfusion in Clinical MedicineFrom EverandMollison's Blood Transfusion in Clinical MedicineRating: 4.5 out of 5 stars4.5/5 (1)
- Immune Biology of Allogeneic Hematopoietic Stem Cell Transplantation: Models in Discovery and TranslationFrom EverandImmune Biology of Allogeneic Hematopoietic Stem Cell Transplantation: Models in Discovery and TranslationGerard SocieNo ratings yet
- Laboratory Tests To Monitor CMV Infection in Transplant PatientsDocument36 pagesLaboratory Tests To Monitor CMV Infection in Transplant PatientsmateenNo ratings yet
- Human Cytomegalovirus and Kidney Transplantation: A Clinician's UpdateDocument9 pagesHuman Cytomegalovirus and Kidney Transplantation: A Clinician's UpdateFlorinda CarranzaNo ratings yet
- Highly Active Antiretroviral Therapy Associated.7Document5 pagesHighly Active Antiretroviral Therapy Associated.7FrancescFranquesaNo ratings yet
- EBV Virus Causing Infectious MononucleosisDocument21 pagesEBV Virus Causing Infectious MononucleosiskamalNo ratings yet
- R1 InfeDocument8 pagesR1 InfeCarla Paola Cortez PérezNo ratings yet
- Zepatier As An Improved Drug Treatment For Hepatitis C Genotypes 1 and 4Document10 pagesZepatier As An Improved Drug Treatment For Hepatitis C Genotypes 1 and 4api-317047226No ratings yet
- Viral Hepatitis 2015Document54 pagesViral Hepatitis 2015Abdulziz Al-jedaieNo ratings yet
- Acute Hepatitis+alf 678Document37 pagesAcute Hepatitis+alf 678Sheren GamaleldenNo ratings yet
- Hepatitis C and D: A Guide to Transmission, Pathogenesis, Diagnosis and TreatmentDocument78 pagesHepatitis C and D: A Guide to Transmission, Pathogenesis, Diagnosis and TreatmentWara RizkyNo ratings yet
- Serology Testing 101: The BasicsDocument49 pagesSerology Testing 101: The Basicsdjf412No ratings yet
- Tests For Dengue GROUP 3Document22 pagesTests For Dengue GROUP 3chocoholic potchiNo ratings yet
- CMV Infection Guide: Symptoms, Diagnosis and TreatmentDocument3 pagesCMV Infection Guide: Symptoms, Diagnosis and TreatmentLucky PuspitasariNo ratings yet
- Hepatitis A-E Viruses: An OverviewDocument48 pagesHepatitis A-E Viruses: An OverviewPrajakta TawdeNo ratings yet
- Immunology 1Document9 pagesImmunology 1Alexandra Duque-DavidNo ratings yet
- Hepatology MRCP1Document87 pagesHepatology MRCP1Raouf Ra'fat SolimanNo ratings yet
- South Africa CMV Viral Load Testing May2015Document4 pagesSouth Africa CMV Viral Load Testing May2015EnergadeNo ratings yet
- ContentServer - Asp 47Document8 pagesContentServer - Asp 47TataNo ratings yet
- Cytomegalovirus (CMV) HepatitisDocument3 pagesCytomegalovirus (CMV) HepatitisN NwekeNo ratings yet
- Cytomegalovirus Prophylaxis With Valganciclovir in Cytomegalovirus-Seropositive Kidney-Transplant PatientsDocument5 pagesCytomegalovirus Prophylaxis With Valganciclovir in Cytomegalovirus-Seropositive Kidney-Transplant PatientspicapicapicapedroNo ratings yet
- South African Hepatitis C Management Guidelines 2010Document18 pagesSouth African Hepatitis C Management Guidelines 2010RatnaSuryatiNo ratings yet
- Citomegalovirus en PostranplantadosDocument26 pagesCitomegalovirus en PostranplantadosJC ChafloqueNo ratings yet
- CitomegalovirusDocument6 pagesCitomegalovirusNebly Cueva JNo ratings yet
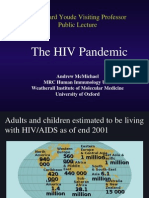
- The HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureDocument50 pagesThe HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureSanthosh SubramanianNo ratings yet
- Window Period Surface Antigen The One That Binds To Receptor in Hepatocytes Anti HBC Not Enough To Clear Infection Hbeag Soluble AntigenDocument22 pagesWindow Period Surface Antigen The One That Binds To Receptor in Hepatocytes Anti HBC Not Enough To Clear Infection Hbeag Soluble AntigenNabelle MarieNo ratings yet
- Digestive Disorders in Children: An Overview of Hepatitis and Liver DiseaseDocument50 pagesDigestive Disorders in Children: An Overview of Hepatitis and Liver DiseaseSven OrdanzaNo ratings yet
- Screening For Hepatitis C Virus InfectionDocument16 pagesScreening For Hepatitis C Virus InfectionFaisal JamshedNo ratings yet
- Infectious Diseases: Hepatitis C Virus Core Antigen Assay: Can We Think Beyond Convention in Resource Limited Settings?Document6 pagesInfectious Diseases: Hepatitis C Virus Core Antigen Assay: Can We Think Beyond Convention in Resource Limited Settings?Lee-Ya AchmadNo ratings yet
- Hepatitis B CronicaDocument11 pagesHepatitis B CronicaMauricio ReinosoNo ratings yet
- Viral HepatitisDocument49 pagesViral HepatitisAster WidodoNo ratings yet
- HIV&liverDocument70 pagesHIV&liverdody_toty278No ratings yet
- Viral Hepatitis Cleveland ClinicsDocument22 pagesViral Hepatitis Cleveland ClinicsWalter FonsecaNo ratings yet
- Hepatology: Gatot Sugiharto, MD, Internist Faculty of Medicine, UWKS Lecture - 2013Document50 pagesHepatology: Gatot Sugiharto, MD, Internist Faculty of Medicine, UWKS Lecture - 2013niluhayusumbawatiNo ratings yet
- Viruses 07 02857Document22 pagesViruses 07 02857Rahmiati LaoNo ratings yet
- Data Evaluation and Reporting BB2803: Elena Chiriac 1420549Document11 pagesData Evaluation and Reporting BB2803: Elena Chiriac 1420549ioana.chiriacNo ratings yet
- Typhoid Fever: Diagnosis Blood and Bone Marrow Culture Faecal and Urine CulturesDocument3 pagesTyphoid Fever: Diagnosis Blood and Bone Marrow Culture Faecal and Urine CulturesDila LarasatiNo ratings yet
- MT 6322 - Mycology and Virology 2nd Shifting OLADocument9 pagesMT 6322 - Mycology and Virology 2nd Shifting OLAlily bluesNo ratings yet
- 13 - Challenges of Monitoring For Treatment FailureDocument34 pages13 - Challenges of Monitoring For Treatment FailureCalvin ChisangoNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument28 pagesDr. Ali's Uworld Notes For Step 2 CKuyesNo ratings yet
- Diagnosis of Hiv Infection BY ThulasiramDocument12 pagesDiagnosis of Hiv Infection BY ThulasiramHareesh ManchikantiNo ratings yet
- FullDocument9 pagesFulldeliaNo ratings yet
- A 1Document5 pagesA 1cikobernicaNo ratings yet
- Lamivudine For Patients With Chronic Hepatitis B and Advanced Liver DiseaseDocument11 pagesLamivudine For Patients With Chronic Hepatitis B and Advanced Liver DiseaseRia DeviNo ratings yet
- Efficacy and Safety of Daclatasvir Plus Sofosbuvir For Treatment-Naïve and Treatment-Experienced Egyptian Patients With Hepatitis C Virus InfectionDocument13 pagesEfficacy and Safety of Daclatasvir Plus Sofosbuvir For Treatment-Naïve and Treatment-Experienced Egyptian Patients With Hepatitis C Virus InfectionIslam NasrNo ratings yet
- Hepatitis B Virus and Hepatitis C Virus Co-Infection With HIVDocument54 pagesHepatitis B Virus and Hepatitis C Virus Co-Infection With HIVShree Narayan YadavNo ratings yet
- Ganciclovir Dosing StrategiesDocument5 pagesGanciclovir Dosing StrategiesLUCY ROSALINOCYNo ratings yet
- EntecavirDocument48 pagesEntecavirAnil RajaniNo ratings yet
- Hepatitis C Virus-Host Interactions and Therapeutics: Current Insights and Future PerspectivesFrom EverandHepatitis C Virus-Host Interactions and Therapeutics: Current Insights and Future PerspectivesNo ratings yet
- Inactive Carriers Who Receive Immunosuppression Should Have Antiviral ProphylaxisDocument3 pagesInactive Carriers Who Receive Immunosuppression Should Have Antiviral ProphylaxisArdy SantosoNo ratings yet
- VDRL Test and Its InterpretationDocument11 pagesVDRL Test and Its InterpretationSauZen SalaZarNo ratings yet
- Virus ChartDocument18 pagesVirus Chartezaz000No ratings yet
- Viral Diagnostic Tests GuideDocument4 pagesViral Diagnostic Tests GuideIeien MuthmainnahNo ratings yet
- Laboratory Diagnosis of HIV Infection: Kamal KishoreDocument7 pagesLaboratory Diagnosis of HIV Infection: Kamal KishoreanastasialantangNo ratings yet
- Hepatitis A-E Viruses: Ni Putu Galuh Wibhutisari (10-169)Document49 pagesHepatitis A-E Viruses: Ni Putu Galuh Wibhutisari (10-169)Echa Anskariani Jon PutriNo ratings yet
- Tacke2016 - Treatment For Hepatitis B in Patients With Drug ResistanceDocument7 pagesTacke2016 - Treatment For Hepatitis B in Patients With Drug ResistanceClarisa AnindyaNo ratings yet
- Virologic Tools For HCV Drug Resistance Testing: Slim Fourati and Jean-Michel PawlotskyDocument14 pagesVirologic Tools For HCV Drug Resistance Testing: Slim Fourati and Jean-Michel Pawlotskyapi-206282033No ratings yet
- Anorectal MalformationDocument17 pagesAnorectal MalformationSilvester SikoraNo ratings yet
- Wa0007.Document47 pagesWa0007.KARLA JOHANNA TARIRA BARROSONo ratings yet
- JurdingDocument19 pagesJurdingifaans16No ratings yet
- Cardiac Arrhythmias Guide - Causes, Symptoms and Treatment OptionsDocument5 pagesCardiac Arrhythmias Guide - Causes, Symptoms and Treatment OptionsaksinuNo ratings yet
- Couden - Community Health Promotion PaperDocument11 pagesCouden - Community Health Promotion Paperapi-449016836No ratings yet
- TMA Letter To Full House SB 5 HB 60Document2 pagesTMA Letter To Full House SB 5 HB 60Drew KochNo ratings yet
- Muhamad Lutfi ParatuberculosisJournalDocument17 pagesMuhamad Lutfi ParatuberculosisJournalLutfi AlkaNo ratings yet
- Vyr GBL 2100296 Seven Ventilators Challenged With Leaks During Neonatal Nasal Cpap - Final - 0Document2 pagesVyr GBL 2100296 Seven Ventilators Challenged With Leaks During Neonatal Nasal Cpap - Final - 0Michael LevitNo ratings yet
- Study of Hemotologicalprofile and Serum Iron Indices in Chronic Kidney Disease in Tertiary Care CentreDocument5 pagesStudy of Hemotologicalprofile and Serum Iron Indices in Chronic Kidney Disease in Tertiary Care CentreIJAR JOURNALNo ratings yet
- Prescription WritingDocument28 pagesPrescription WritingEshana AryaNo ratings yet
- Chapter 038Document63 pagesChapter 038Mackenzie MartiniNo ratings yet
- Medical Device Risk Classification GuidanceDocument36 pagesMedical Device Risk Classification GuidanceGina ArcNo ratings yet
- Infinity Omega S Solution BR 9051850 en GBDocument12 pagesInfinity Omega S Solution BR 9051850 en GBJustiniano MartelNo ratings yet
- Distal Tibial Fractures Intramedullary NailingDocument8 pagesDistal Tibial Fractures Intramedullary NailingasdaadNo ratings yet
- Subcutaneous Herniation of Fetuses After Blunt Force Trauma in A CatDocument4 pagesSubcutaneous Herniation of Fetuses After Blunt Force Trauma in A CatTatiana Amaya GomezNo ratings yet
- A Treatise On Advance Acupressure/Acupuncture (Part Xiii) - Kidney & Urinary Tract Disorders Efje Eùeeveg EâceefcekeâeDocument19 pagesA Treatise On Advance Acupressure/Acupuncture (Part Xiii) - Kidney & Urinary Tract Disorders Efje Eùeeveg EâceefcekeâeParvathy ShekharNo ratings yet
- Massive Transfusion and Massive Transfusion ProtocolDocument9 pagesMassive Transfusion and Massive Transfusion ProtocolRamachandran SundararamanNo ratings yet
- Otitis Media: Prepared By: - Priyanka ThapaDocument38 pagesOtitis Media: Prepared By: - Priyanka ThapaKalo kajiNo ratings yet
- World Alzheimer Report 2022Document416 pagesWorld Alzheimer Report 2022bowman1977No ratings yet
- Pediatricians' Letter To LCS Superintendent Rocky HannaDocument2 pagesPediatricians' Letter To LCS Superintendent Rocky HannaWCTV Digital TeamNo ratings yet
- BM Project On SpirometerDocument11 pagesBM Project On SpirometerAnushka NardeNo ratings yet
- Diseases of The Pharynx: BY DR Arif Raza Khan Assistant Professor E.N.T. K.T.HDocument29 pagesDiseases of The Pharynx: BY DR Arif Raza Khan Assistant Professor E.N.T. K.T.HSuleman MuhammadNo ratings yet
- Schedule Ismi HottiDocument23 pagesSchedule Ismi HottisigitNo ratings yet